

Intestinal Microbiome Changes in Fecal Microbiota Transplant (FMT) vs. FMT Enriched with Lactobacillus in the Treatment of Recurrent Clostridioides difficile Infection
- PMID: 31976311
- PMCID: PMC6955117
- DOI: 10.1155/2019/4549298
Intestinal Microbiome Changes in Fecal Microbiota Transplant (FMT) vs. FMT Enriched with Lactobacillus in the Treatment of Recurrent Clostridioides difficile Infection
Abstract
Aim: In this study, we conducted a comparative study to explore the differences in therapeutic efficacy and intestinal microbiome of fecal microbiota transplant (FMT) vs. FMT in addition with Lactobacillus (FMT-L) for treatment of recurrent Clostridioides difficile infection (R-CDI).
Methods: We designed a double-blinded randomized comparative two-arm pilot multicenter study to assess the efficacy and impact in the intestinal microbiome of standard capsules of FMT vs. FMT-L enriched with 3 species of Lactobacillus for patients with R-CDI. A 90-day follow-up of 21 patients was performed, starting at the beginning of the study. From the selected patients, fecal samples were obtained at days 0, 3, 7, and 28 after treatment. Fecal samples and FMT were analyzed by 16S rRNA sequencing.
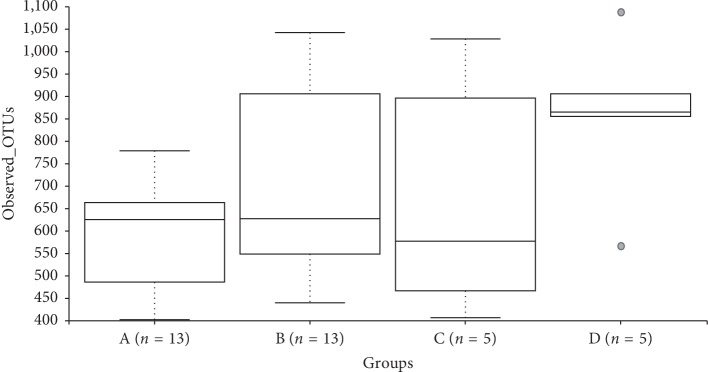
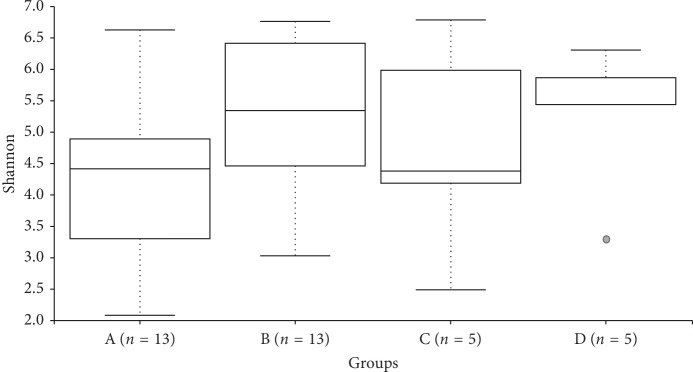
Results: We included 21 patients (13 in the FMT group and 8 in the FMT-L group). Overall, both groups had a reduction in bowel movements per day, from 8.6 to 3.2 in the first 48 h (62.7% reduction, p=0.001). No severe adverse reactions or recurrences were recorded. Firmicutes were the most abundant phylum in donors. A low relative abundance of Proteobacteria was detected and mostly found in patients even at higher proportions than the donor. The donor's pool also had relatively few Bacteroidetes, and some patients showed a higher abundance of this phylum. Based on the ANOSIM R values, there is a significant difference between the microbial communities of basal samples and samples collected on day 7 (p=0.045) and at day 28 (0.041).
Conclusion: Fecal microbiota transplant by capsules was clinically and genomically similar between traditional FMT and enriched FMT with Lactobacillus spp. Restoration of bacterial diversity and resolution of dysbiosis at days 7 and 28 were observed. Patients with a first episode of recurrence treated with FMT had an excellent response without severe adverse events; FMT should be considered as an early treatment during R-CDI.
Copyright © 2019 Elvira Garza-González et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures



References
-
- Clifford McDonald L., Gerding D. N., Johnson S., et al. Clinical practice guidelines for clostridium difficile infection in adults and children: 2017 update by the infectious diseases society of America (IDSA) and society for healthcare epidemiology of America (SHEA) Clinical Infectious Diseases. 2018;66(7):e1–e48. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
