

Randomized, Multicenter, Phase II Trial of Gemcitabine and Cisplatin With or Without Veliparib in Patients With Pancreas Adenocarcinoma and a Germline BRCA/PALB2 Mutation
- PMID: 31976786
- PMCID: PMC7193749
- DOI: 10.1200/JCO.19.02931
Randomized, Multicenter, Phase II Trial of Gemcitabine and Cisplatin With or Without Veliparib in Patients With Pancreas Adenocarcinoma and a Germline BRCA/PALB2 Mutation
Abstract
Purpose: Five percent to 9% of pancreatic ductal adenocarcinomas (PDACs) develop in patients with a germline BRCA1/2 or PALB2 (gBRCA/PALB2+) mutation. Phase IB data from a trial that used cisplatin, gemcitabine, and veliparib treatment demonstrated a high response rate (RR), disease control rate (DCR), and overall survival (OS) in this population. We designed an open-label, randomized, multicenter, two-arm phase II trial to investigate cisplatin and gemcitabine with or without veliparib in gBRCA/PALB2+ PDAC.
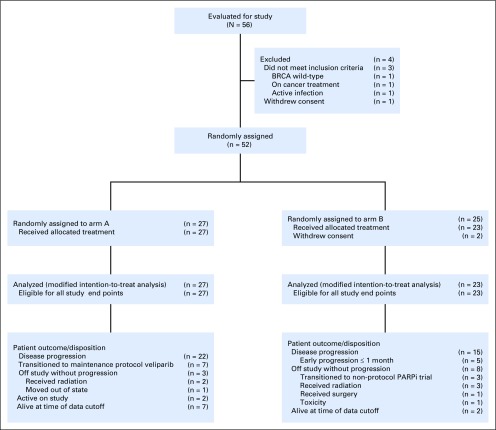
Patients and methods: Eligible patients had untreated gBRCA/PALB2+ PDAC with measurable stage III to IV disease and Eastern Cooperative Oncology Group performance status of 0 to 1. Treatment for patients in arm A consisted of cisplatin 25 mg/m2 and gemcitabine 600 mg/m2 intravenously on days 3 and 10; treatment for patients in arm B was the same as that for patients in arm A, and arm A also received veliparib 80 mg orally twice per day on days 1 to 12 cycled every 3 weeks. The primary end point was RRs of arm A and arm B evaluated separately using a Simon two-stage design. Secondary end points were progression-free survival, DCR, OS, safety, and correlative analyses.
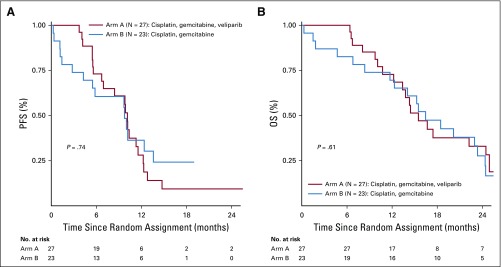
Results: Fifty patients were evaluated by modified intention-to-treat analysis. The RR for arm A was 74.1% and 65.2% for arm B (P = .55); both arms exceeded the prespecified activity threshold. DCR was 100% for arm A and 78.3% for arm B (P = .02). Median progression-free survival was 10.1 months for arm A (95% CI, 6.7 to 11.5 months) and 9.7 months for arm B (95% CI, 4.2 to 13.6 months; P = .73). Median OS for arm A was 15.5 months (95% CI, 12.2 to 24.3 months) and 16.4 months for arm B (95% CI, 11.7 to 23.4 months; P = .6). Two-year OS rate for the entire cohort was 30.6% (95% CI, 17.8% to 44.4%), and 3-year OS rate was 17.8% (95% CI, 8.1% to 30.7%). Grade 3 to 4 hematologic toxicities for arm A versus arm B were 13 (48%) versus seven (30%) for neutropenia, 15 (55%) versus two (9%) for thrombocytopenia, and 14 (52%) versus eight (35%) for anemia.
Conclusion: Cisplatin and gemcitabine is an effective regimen in advanced gBRCA/PALB2+ PDAC. Concurrent veliparib did not improve RR. These data establish cisplatin and gemcitabine as a standard approach in gBRCA/PALB2+ PDAC.
Figures

Comment in
-
Cisplatin Plus Gemcitabine as Standard of Care for Germline BRCA/PALB2-Mutated Pancreatic Adenocarcinoma: Are We Moving Too Fast?J Clin Oncol. 2020 Jul 20;38(21):2466-2467. doi: 10.1200/JCO.20.00419. Epub 2020 May 14. J Clin Oncol. 2020. PMID: 32407212 No abstract available.
-
Reply to N. Fazio.J Clin Oncol. 2020 Jul 20;38(21):2467-2468. doi: 10.1200/JCO.20.00833. Epub 2020 May 14. J Clin Oncol. 2020. PMID: 32407214 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
