

Ovarian-Adnexal Reporting Data System Magnetic Resonance Imaging (O-RADS MRI) Score for Risk Stratification of Sonographically Indeterminate Adnexal Masses
- PMID: 31977064
- PMCID: PMC6991280
- DOI: 10.1001/jamanetworkopen.2019.19896
Ovarian-Adnexal Reporting Data System Magnetic Resonance Imaging (O-RADS MRI) Score for Risk Stratification of Sonographically Indeterminate Adnexal Masses
Abstract
Importance: Approximately one-quarter of adnexal masses detected at ultrasonography are indeterminate for benignity or malignancy, posing a substantial clinical dilemma.
Objective: To validate the accuracy of a 5-point Ovarian-Adnexal Reporting Data System Magnetic Resonance Imaging (O-RADS MRI) score for risk stratification of adnexal masses.
Design, setting, and participants: This multicenter cohort study was conducted between March 1, 2013, and March 31, 2016. Among patients undergoing expectant management, 2-year follow-up data were completed by March 31, 2018. A routine pelvic MRI was performed among consecutive patients referred to characterize a sonographically indeterminate adnexal mass according to routine diagnostic practice at 15 referral centers. The MRI score was prospectively applied by 2 onsite readers and by 1 reader masked to clinical and ultrasonographic data. Data analysis was conducted between April and November 2018.
Main outcomes and measures: The primary end point was the joint analysis of true-negative and false-negative rates according to the MRI score compared with the reference standard (ie, histology or 2-year follow-up).
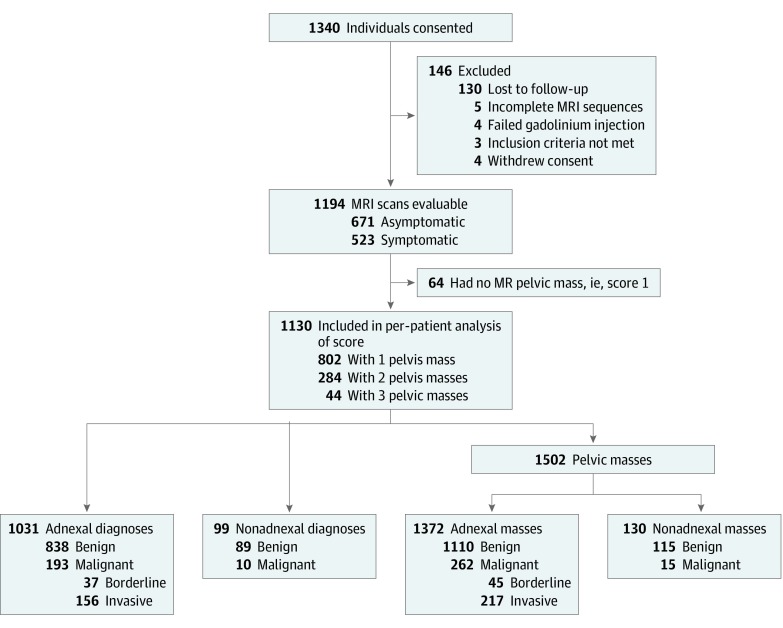
Results: A total of 1340 women (mean [range] age, 49 [18-96] years) were enrolled. Of 1194 evaluable women, 1130 (94.6%) had a pelvic mass on MRI with a reference standard (surgery, 768 [67.9%]; 2-year follow-up, 362 [32.1%]). A total of 203 patients (18.0%) had at least 1 malignant adnexal or nonadnexal pelvic mass. No invasive cancer was assigned a score of 2. Positive likelihood ratios were 0.01 for score 2, 0.27 for score 3, 4.42 for score 4, and 38.81 for score 5. Area under the receiver operating characteristic curve was 0.961 (95% CI, 0.948-0.971) among experienced readers, with a sensitivity of 0.93 (95% CI, 0.89-0.96; 189 of 203 patients) and a specificity of 0.91 (95% CI, 0.89-0.93; 848 of 927 patients). There was good interrater agreement among both experienced and junior readers (κ = 0.784; 95% CI, 0.743-0824). Of 580 of 1130 women (51.3%) with a mass on MRI and no specific gynecological symptoms, 362 (62.4%) underwent surgery. Of them, 244 (67.4%) had benign lesions and a score of 3 or less. The MRI score correctly reclassified the mass origin as nonadnexal with a sensitivity of 0.99 (95% CI, 0.98-0.99; 1360 of 1372 patients) and a specificity of 0.78 (95% CI, 0.71-0.85; 102 of 130 patients).
Conclusions and relevance: In this study, the O-RADS MRI score was accurate when stratifying the risk of malignancy in adnexal masses.
Conflict of interest statement
Figures
Comment in
-
Performance of O-RADS MRI Score for Classifying Indeterminate Adnexal Masses at US.Radiol Imaging Cancer. 2021 May;3(3):e219008. doi: 10.1148/rycan.2021219008. Radiol Imaging Cancer. 2021. PMID: 34047668 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
