

Review
doi: 10.2106/JBJS.19.00591.
Necrotizing Fasciitis: Pillaging the Acute Phase Response
Affiliations
- PMID: 31977818
- PMCID: PMC8590823
- DOI: 10.2106/JBJS.19.00591
Item in Clipboard
Review
Necrotizing Fasciitis: Pillaging the Acute Phase Response
J Bone Joint Surg Am.
.
No abstract available
Figures
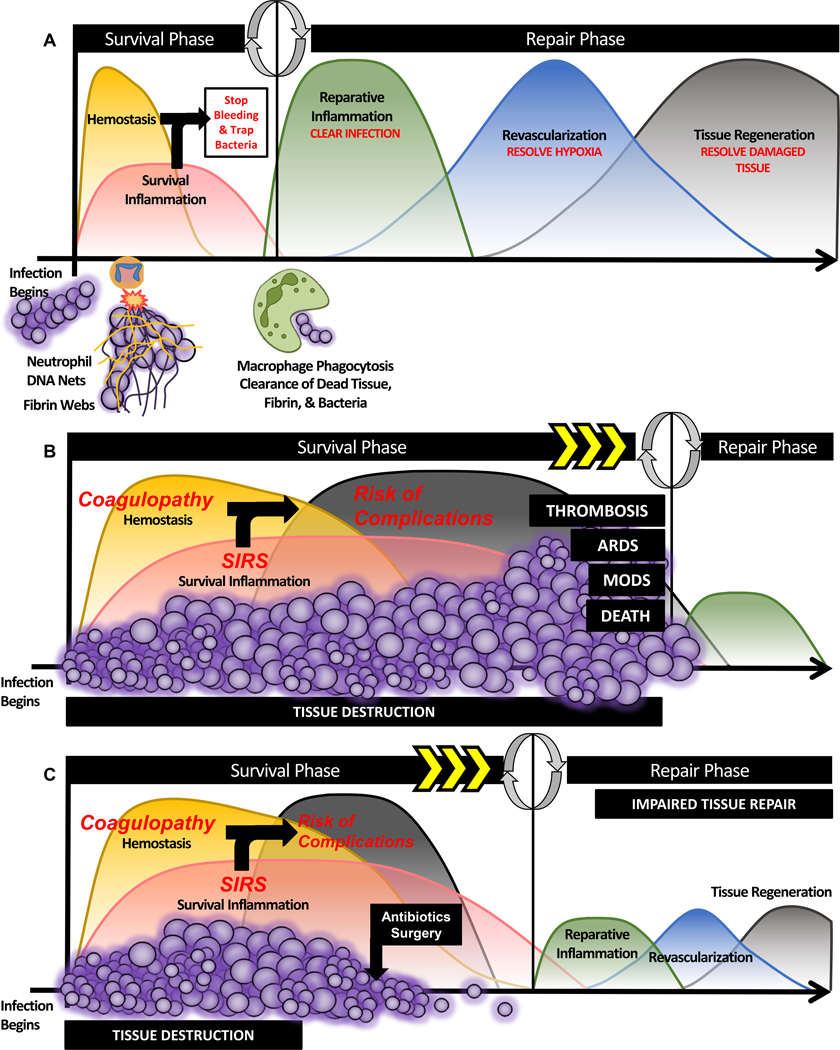
Figs. 1-A, 1-B, and 1-C The acute phase response, the body’s response to infection and associated tissue destruction. (Published with permission of Jonathan G. Schoenecker, MD, PhD.) Fig. 1-A Following the establishment of an infection and the associated tissue destruction, the body must first resolve bleeding and contain the bacteria (neutrophil-derived DNA nets and fibrin webs) to reduce further tissue damage. Together, hemostasis and the survival inflammatory response comprise the survival phase of the acute phase response, which together are essential to preserve life. Once bleeding has been stopped and the bacteria are contained, the body can transition to the reparative phase where reparative inflammation components, such as macrophages, can enter the tissue and begin to clear dead cellular debris, bacteria, and the previously established fibrin matrices. Once cleared, revascularization and tissue regeneration of the damaged tissues can occur to reestablish the pre-infection physiologic state. Fig. 1-B However, if the infection is rapidly progressing and highly destructive, such as necrotizing fasciitis, the survival phase of the acute phase response will become exuberantly activated, as it attempts to respond to the progressing infection and tissue destruction. The overexuberant activation of the hemostatic response can result in coagulopathy (SIC) and that of the survival inflammatory response can result in SIRS. Together, time spent under these 2 systemic states increases the patient’s risk for complications such as thrombosis, acute respiratory distress syndrome (ARDS), multi-organ dysfunction syndrome (MODS), and death. Fig. 1-C Given that necrotizing fasciitis is a rapidly progressing infection that causes substantial tissue damage, the survival phase will become exuberantly activated. Yet, through intervention with surgical debridement and antibiotic administration, the pathogen onslaught can be reduced, allowing the survival phase of the acute phase response to be sufficient to stop bleeding and trap the remaining bacteria. However, given the rapid nature of necrotizing fasciitis, tissue destruction is imminent. As patients pass into the repair phase once the infection is cleared, many still experience impaired tissue healing in response to a dysregulated acute phase response.
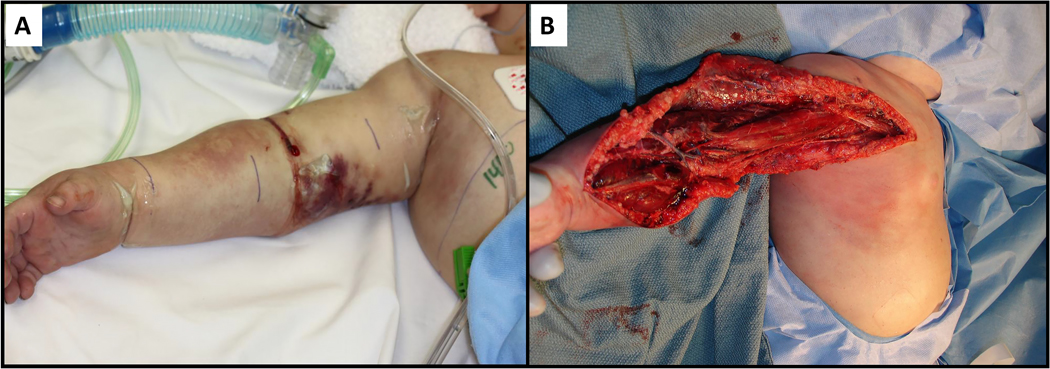
Figs. 2-A and 2-B Clinical presentation and surgical debridement of a pediatric patient with necrotizing fasciitis. Fig. 2-A Appearance of a patient’s arm on presentation with the characteristic findings of necrotizing fasciitis: erysipelas, swelling, discharge, and mottling. Fig. 2-B Intraoperative findings demonstrate the destructive nature of necrotizing fasciitis. Rapid dissemination of bacteria and liquefactive necrosis beneath fascial planes resulted in well-dissected muscular compartments independent of the surgeon’s knife.
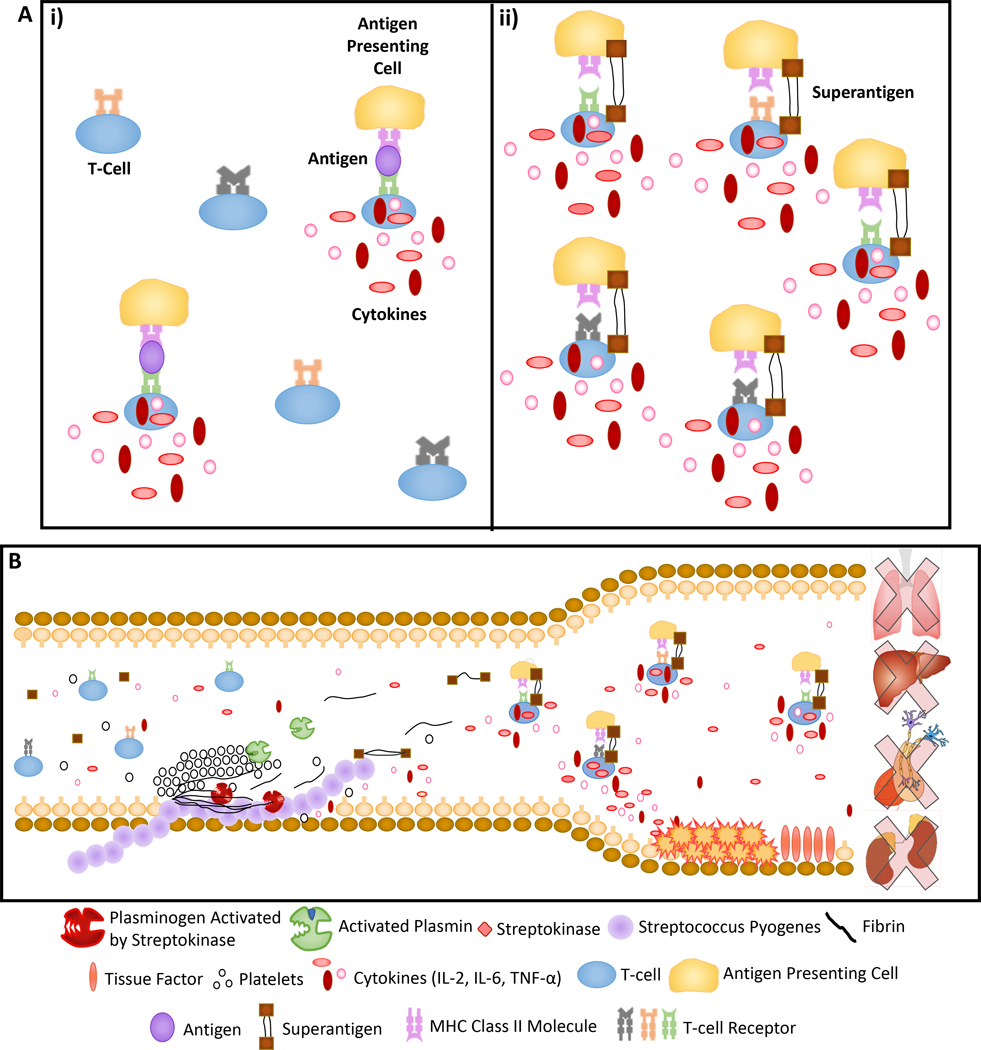
Figs. 3-A and 3-B Release of superantigens and the development of shock in response to infection. Superantigens are a family of proteins that bind major histocompatibility complex (MHC) class-II molecules without first going through the conventional pathways of antigen processing and presentation by antigen presenting cells. This allows superantigens to bind MHC class-II molecules as intact proteins at sites other than the peptide binding groove. (Published with permission of Jonathan G. Schoenecker, MD, PhD.) Fig. 3-A In the body’s normal response to infection, MHC-II mediated presentation of antigens to T-cells results in the release of cytokines and bolsters the immune response (i). Bypassing MHC-restricted antigen processing in this manner, superantigens can activate an abnormally large fraction of host T-cells (up to 25%) and lead to an excessive inflammatory response resulting in septic shock. Fig. 3-B In the setting of necrotizing fasciitis, superantigens produced by Streptococcus pyogenes result in a massive release of cytokines (such as tumor necrosis factor [TNF]-α) into systemic circulation. These cytokines have a number of detrimental effects including widespread vasodilation, disruption of the vascular endothelium, and hypercoagulability (i.e., increased clotting factor production via the liver and upregulated expression of tissue factor on the vascular endothelium). These systemic effects contribute to the septic shock and multi-organ failure that are often the cause of death in patients with necrotizing fasciitis.
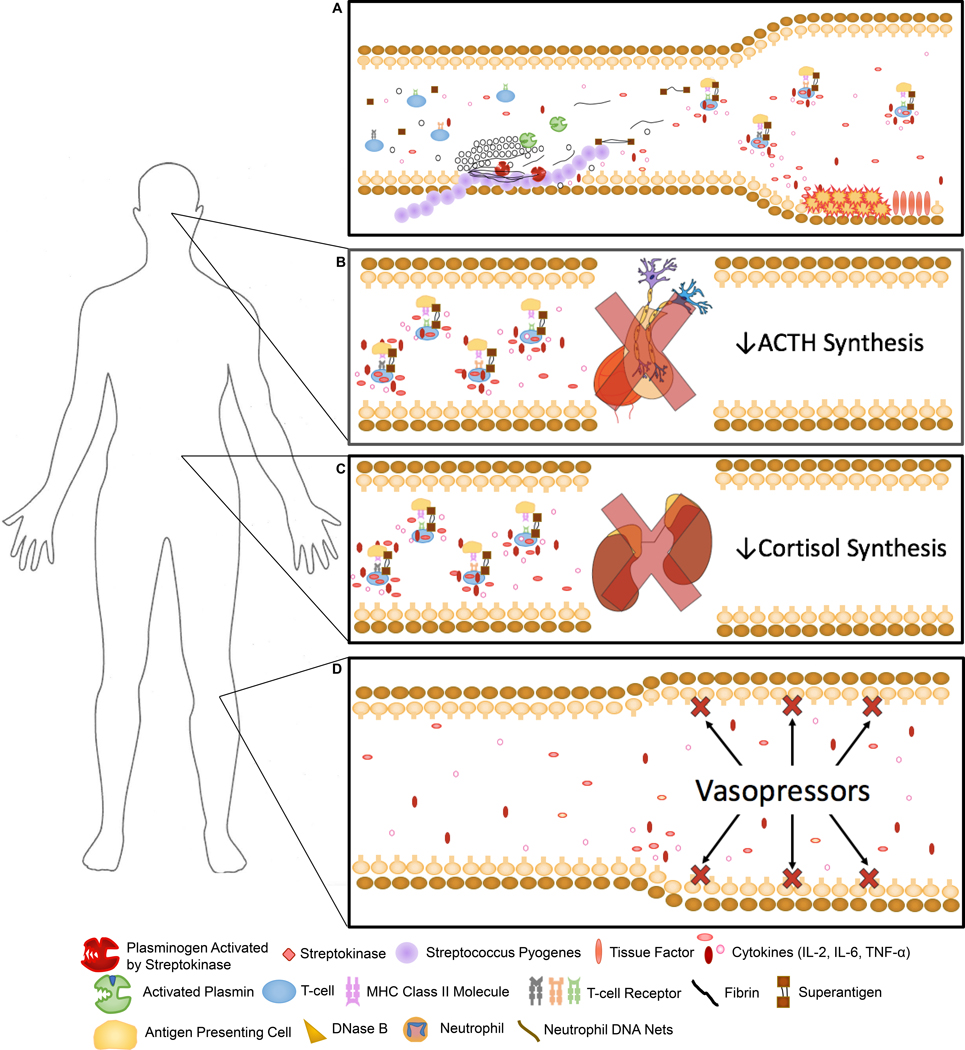
Figs. 4-A through 4-D CIRCI. MHC = major histocompatibility complex and TNF = tumor necrosis factor. (Published with permission of Jonathan G. Schoenecker, MD, PhD.) Fig. 4-A Representative image of streptococcal superantigens leading to the aberrant release of cytokines. These cytokines disseminate systemically, causing hyperinflammation that contributes to vasodilation, tissue damage, and hypercoagulability. Fig. 4-B Hypothalamic or pituitary dysfunction secondary to impaired protein synthesis, hemorrhage, and/or infarction may contribute to CIRCI by reducing the production of ACTH, which, in turn, results in less cortisol production by the adrenal glands. Fig. 4-C Adrenal gland dysfunction secondary to decreased ACTH production by the pituitary gland, impaired cortisol synthesis, hemorrhage, and/or infarction may contribute to CIRCI by direct loss of corticosteroid production. Fig. 4-D This state of relative corticosteroid insufficiency or resistance in conjunction with the vasodilation of toxic shock results in vasopressor-resistant hypotension. If not corrected, end organ damage caused by hypoperfusion can contribute to the mortality of necrotizing fasciitis.
References
-
- Stevens DL, Bryant AE. Necrotizing soft-tissue infections. N Engl J Med. 2017. December 7;377(23):2253–65. - PubMed
-
- An TJ, Benvenuti MA, Mignemi ME, Thomsen IP, Schoenecker JG. Pediatric musculoskeletal infection: hijacking the acute-phase response. JBJS Rev. 2016. September 27;4(9):01874474–201609000-00001. - PubMed
-
- Hippocrates. De morbis popularibus, epidemics III. Harvard University Press; 1868.
-
- Jones J. Investigations upon the nature, causes, and treatments of hospital gangrene, as it prevailed in the Confederate armies, 1861–1865. New York: Surg Mem War Rebellion; 1871.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
