

Lean back and wait for the alarm? Testing an automated alarm system for nosocomial outbreaks to provide support for infection control professionals
- PMID: 31978086
- PMCID: PMC6980399
- DOI: 10.1371/journal.pone.0227955
Lean back and wait for the alarm? Testing an automated alarm system for nosocomial outbreaks to provide support for infection control professionals
Abstract
Introduction: Outbreaks of communicable diseases in hospitals need to be quickly detected in order to enable immediate control. The increasing digitalization of hospital data processing offers potential solutions for automated outbreak detection systems (AODS). Our goal was to assess a newly developed AODS.
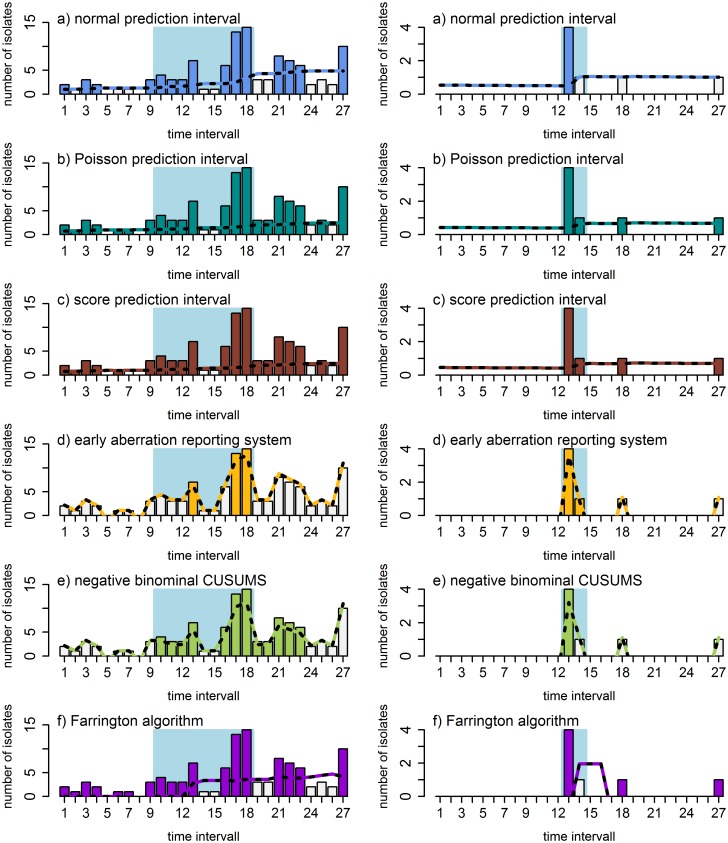
Methods: Our AODS was based on the diagnostic results of routine clinical microbiological examinations. The system prospectively counted detections per bacterial pathogen over time for the years 2016 and 2017. The baseline data covers data from 2013-2015. The comparative analysis was based on six different mathematical algorithms (normal/Poisson and score prediction intervals, the early aberration reporting system, negative binomial CUSUMs, and the Farrington algorithm). The clusters automatically detected were then compared with the results of our manual outbreak detection system.
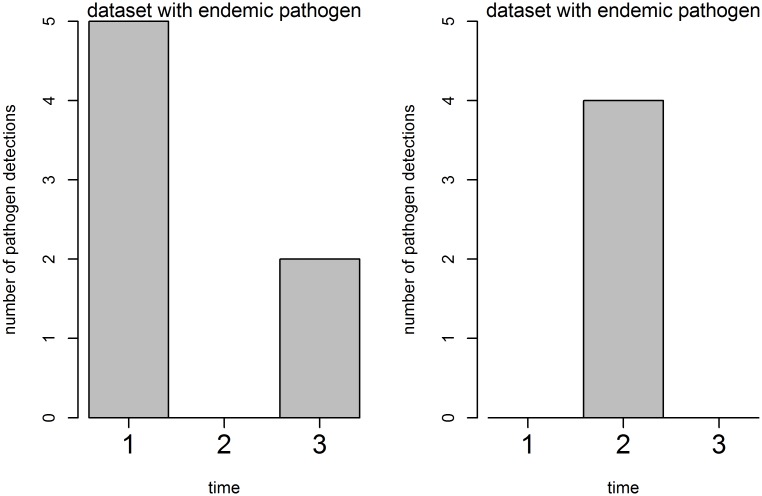
Results: During the analysis period, 14 different hospital outbreaks were detected as a result of conventional manual outbreak detection. Based on the pathogens' overall incidence, outbreaks were divided into two categories: outbreaks with rarely detected pathogens (sporadic) and outbreaks with often detected pathogens (endemic). For outbreaks with sporadic pathogens, the detection rate of our AODS ranged from 83% to 100%. Every algorithm detected 6 of 7 outbreaks with a sporadic pathogen. The AODS identified outbreaks with an endemic pathogen were at a detection rate of 33% to 100%. For endemic pathogens, the results varied based on the epidemiological characteristics of each outbreak and pathogen.
Conclusion: AODS for hospitals based on routine microbiological data is feasible and can provide relevant benefits for infection control teams. It offers in-time automated notification of suspected pathogen clusters especially for sporadically occurring pathogens. However, outbreaks of endemically detected pathogens need further individual pathogen-specific and setting-specific adjustments.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Automated detection of outbreaks of antimicrobial-resistant bacteria in Japan.J Hosp Infect. 2019 Jun;102(2):226-233. doi: 10.1016/j.jhin.2018.10.005. Epub 2018 Oct 12. J Hosp Infect. 2019. PMID: 30321629 Free PMC article.
-
Differential impact of infection control strategies on rates of resistant hospital-acquired pathogens in critically ill surgical patients.Surg Infect (Larchmt). 2014 Dec;15(6):726-32. doi: 10.1089/sur.2013.265. Surg Infect (Larchmt). 2014. PMID: 25496277
-
Automated detection of infectious disease outbreaks in hospitals: a retrospective cohort study.PLoS Med. 2010 Feb 23;7(2):e1000238. doi: 10.1371/journal.pmed.1000238. PLoS Med. 2010. PMID: 20186274 Free PMC article.
-
Outbreaks of nosocomial infections: lessons learned and perspectives.Curr Opin Infect Dis. 2008 Aug;21(4):357-61. doi: 10.1097/QCO.0b013e3283013933. Curr Opin Infect Dis. 2008. PMID: 18594286 Review.
-
Epidemiology as a tool for hospital infection control.Acta Clin Belg. 1998 Apr;53(2):75-82. doi: 10.1080/17843286.1998.11754147. Acta Clin Belg. 1998. PMID: 9639944 Review.
Cited by
-
Prevalence and risk factors of colonisation with vancomycin-resistant Enterococci faecium upon admission to Germany's largest university hospital.GMS Hyg Infect Control. 2021 Jan 29;16:Doc06. doi: 10.3205/dgkh000377. eCollection 2021. GMS Hyg Infect Control. 2021. PMID: 33643773 Free PMC article.
-
Transformation of microbiology data into a standardised data representation using OpenEHR.Sci Rep. 2021 May 18;11(1):10556. doi: 10.1038/s41598-021-89796-y. Sci Rep. 2021. PMID: 34006956 Free PMC article.
-
An openEHR based infection control system to support monitoring of nosocomial bacterial clusters and contacts.NPJ Digit Med. 2025 Jun 30;8(1):385. doi: 10.1038/s41746-025-01795-9. NPJ Digit Med. 2025. PMID: 40588668 Free PMC article.
-
Early warning for healthcare acquired infections in neonatal care units in a low-resource setting using routinely collected hospital data: The experience from Haiti, 2014-2018.PLoS One. 2022 Jun 23;17(6):e0269385. doi: 10.1371/journal.pone.0269385. eCollection 2022. PLoS One. 2022. PMID: 35737713 Free PMC article.
-
Corticosteroids as risk factor for COVID-19-associated pulmonary aspergillosis in intensive care patients.Crit Care. 2022 Jan 28;26(1):30. doi: 10.1186/s13054-022-03902-8. Crit Care. 2022. PMID: 35090528 Free PMC article.
References
-
- Bergin SM, Periaswamy B, Barkham T, Chua HC, Mok YM, Fung DSS, et al. An Outbreak of Streptococcus pyogenes in a Mental Health Facility: Advantage of Well-Timed Whole-Genome Sequencing Over emm Typing. Infection control and hospital epidemiology. 2018:1–9. - PubMed
-
- Baker MA, Huang SS, Letourneau AR, Kaganov RE, Peeples JR, Drees M, et al. Lack of comprehensive outbreak detection in hospitals. infection control & hospital epidemiology. 2016;37(4):466–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
