

ACL reconstruction combined with lateral monoloop tenodesis can restore intact knee laxity
- PMID: 31980844
- PMCID: PMC7148266
- DOI: 10.1007/s00167-019-05839-y
ACL reconstruction combined with lateral monoloop tenodesis can restore intact knee laxity
Abstract
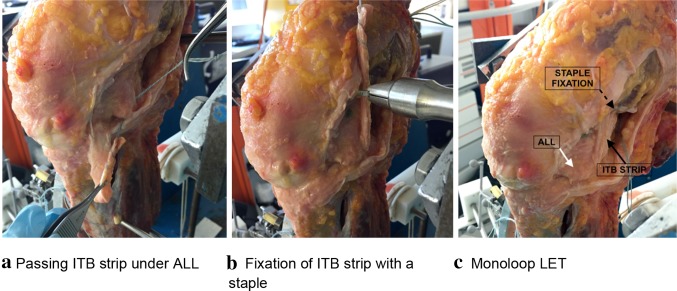
Purpose: An anterior cruciate ligament (ACL) injury is often combined with injury to the lateral extra-articular structures, which may cause a combined anterior and rotational laxity. It was hypothesised that addition of a 'monoloop' lateral extra-articular tenodesis (mLET) to an ACL reconstruction would restore anteroposterior, internal rotation and pivot-shift laxities better than isolated ACL reconstruction in combined injuries.
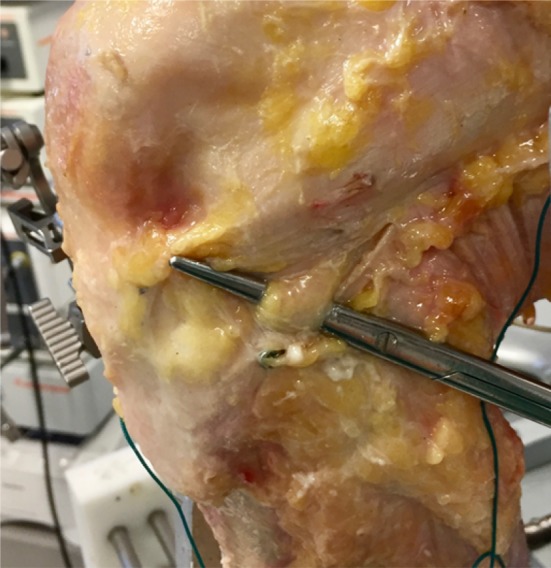
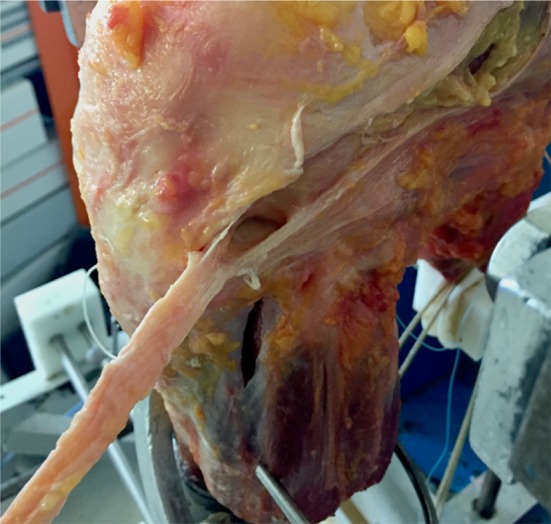
Method: Twelve cadaveric knees were tested, using an optical tracking system to record the kinematics through 0°-100° of knee flexion with no load, anterior and posterior translational forces (90 N), internal and external rotational torques (5 Nm), and a combination of an anterior translational (90 N) plus internal rotational load (5 Nm). They were tested intact, after sectioning the ACL, sectioning anterolateral ligament (ALL), iliotibial band (ITB) graft harvest, releasing deep ITB fibres, hamstrings tendon ACL reconstruction, mLET combined with ACL reconstruction, and isolated mLET. Two-way repeated-measures ANOVA compared laxity data across knee states and flexion angles. When differences were found, paired t tests with Bonferroni correction were performed.
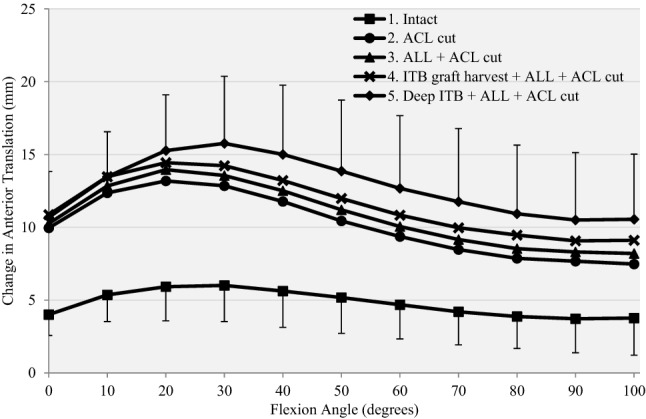
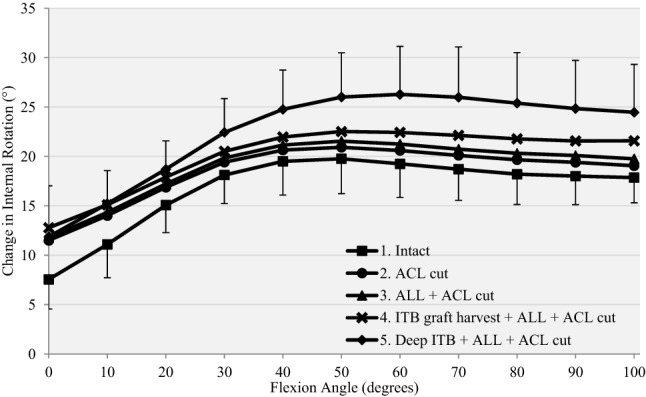
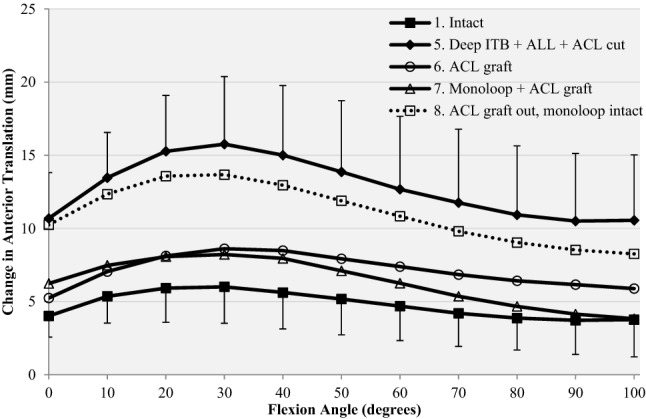
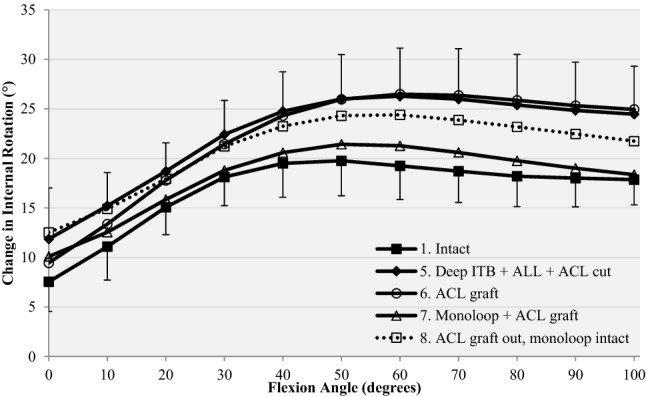
Results: In the ACL-deficient knee, cutting the ALL significantly increased anterior laxity only at 20°-30°, and only significantly increased internal rotation at 50°. Additional deep ITB release significantly increased anterior laxity at 40°-90° and caused a large increase of internal rotation at 20°-100°. Isolated ACL reconstruction restored anterior drawer, but significant differences remained in internal rotation at 30°-100°. After adding an mLET there were no remaining differences with anterior translation or internal rotation compared to the intact knee. With the combined injury, isolated mLET allowed abnormal anterior translation and rotation to persist.
Conclusions: Cutting the deep fibres of the ITB caused large increases in tibial internal rotation laxity across the range of knee flexion, while cutting the ALL alone did not. With ACL deficiency combined with anterolateral deficiency, ACL reconstruction alone was insufficient to restore native knee rotational laxity. However, combining a 'monoloop' lateral extra-articular tenodesis with ACL reconstruction did restore native knee laxity.
Keywords: ACL reconstruction; Anterolateral rotational instability; Biomechanics; Knee laxity; Lateral extra-articular tenodesis; Monoloop.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Amirault JD, Cameron JC, MacIntosh DL, Marks P. Chronic anterior cruciate ligament deficiency. Long-term results of MacIntosh's lateral substitution reconstruction. J Bone Jt Surg Br. 1988;70(4):622–624. - PubMed
-
- Amis AA, Scammell BE. Biomechanics of intra-articular and extra-articular reconstruction of the anterior cruciate ligament. J Bone Jt Surg Br. 1993;75:812–817. - PubMed
-
- Bull AM, Earnshaw PH, Smith A, Katchburian MV, Hassan AN, Amis AA. Intraoperative measurement of knee kinematics in reconstruction of the anterior cruciate ligament. J Bone Jt Surg Br. 2002;84(7):1075–1081. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
