

Efficacy of three neuroprotective drugs in secondary progressive multiple sclerosis (MS-SMART): a phase 2b, multiarm, double-blind, randomised placebo-controlled trial
- PMID: 31981516
- PMCID: PMC7029307
- DOI: 10.1016/S1474-4422(19)30485-5
Efficacy of three neuroprotective drugs in secondary progressive multiple sclerosis (MS-SMART): a phase 2b, multiarm, double-blind, randomised placebo-controlled trial
Abstract
Background: Neurodegeneration is the pathological substrate that causes major disability in secondary progressive multiple sclerosis. A synthesis of preclinical and clinical research identified three neuroprotective drugs acting on different axonal pathobiologies. We aimed to test the efficacy of these drugs in an efficient manner with respect to time, cost, and patient resource.
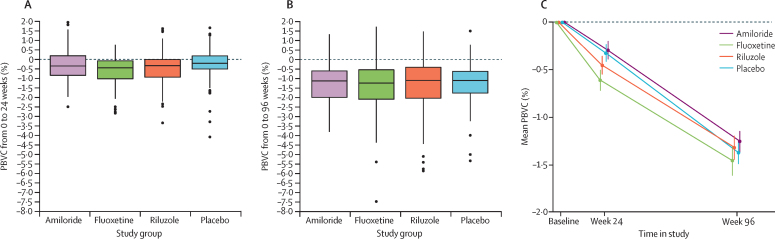
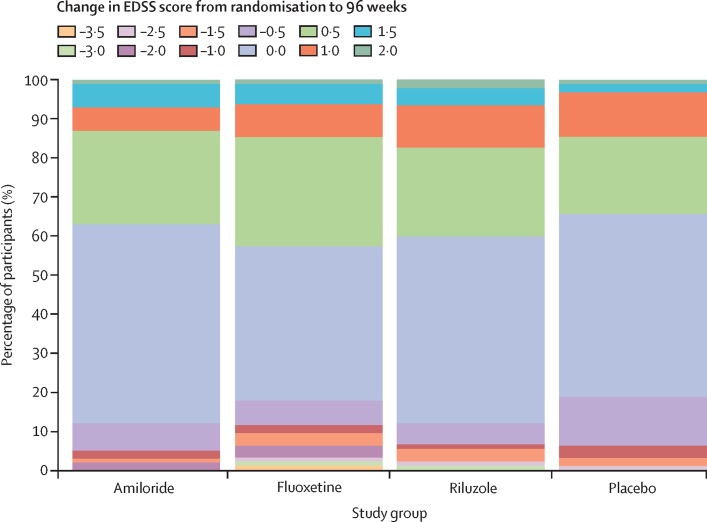
Methods: We did a phase 2b, multiarm, parallel group, double-blind, randomised placebo-controlled trial at 13 clinical neuroscience centres in the UK. We recruited patients (aged 25-65 years) with secondary progressive multiple sclerosis who were not on disease-modifying treatment and who had an Expanded Disability Status Scale (EDSS) score of 4·0-6·5. Participants were randomly assigned (1:1:1:1) at baseline, by a research nurse using a centralised web-based service, to receive twice-daily oral treatment of either amiloride 5 mg, fluoxetine 20 mg, riluzole 50 mg, or placebo for 96 weeks. The randomisation procedure included minimisation based on sex, age, EDSS score at randomisation, and trial site. Capsules were identical in appearance to achieve masking. Patients, investigators, and MRI readers were unaware of treatment allocation. The primary outcome measure was volumetric MRI percentage brain volume change (PBVC) from baseline to 96 weeks, analysed using multiple regression, adjusting for baseline normalised brain volume and minimisation criteria. The primary analysis was a complete-case analysis based on the intention-to-treat population (all patients with data at week 96). This trial is registered with ClinicalTrials.gov, NCT01910259.
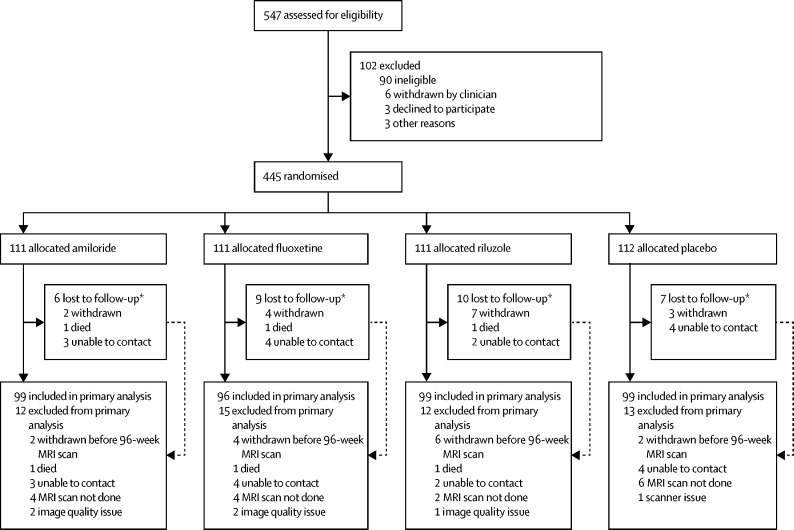
Findings: Between Jan 29, 2015, and June 22, 2016, 445 patients were randomly allocated amiloride (n=111), fluoxetine (n=111), riluzole (n=111), or placebo (n=112). The primary analysis included 393 patients who were allocated amiloride (n=99), fluoxetine (n=96), riluzole (n=99), and placebo (n=99). No difference was noted between any active treatment and placebo in PBVC (amiloride vs placebo, 0·0% [95% CI -0·4 to 0·5; p=0·99]; fluoxetine vs placebo -0·1% [-0·5 to 0·3; p=0·86]; riluzole vs placebo -0·1% [-0·6 to 0·3; p=0·77]). No emergent safety issues were reported. The incidence of serious adverse events was low and similar across study groups (ten [9%] patients in the amiloride group, seven [6%] in the fluoxetine group, 12 [11%] in the riluzole group, and 13 [12%] in the placebo group). The most common serious adverse events were infections and infestations. Three patients died during the study, from causes judged unrelated to active treatment; one patient assigned amiloride died from metastatic lung cancer, one patient assigned riluzole died from ischaemic heart disease and coronary artery thrombosis, and one patient assigned fluoxetine had a sudden death (primary cause) with multiple sclerosis and obesity listed as secondary causes.
Interpretation: The absence of evidence for neuroprotection in this adequately powered trial indicates that exclusively targeting these aspects of axonal pathobiology in patients with secondary progressive multiple sclerosis is insufficient to mitigate neuroaxonal loss. These findings argue for investigation of different mechanistic targets and future consideration of combination treatment trials. This trial provides a template for future simultaneous testing of multiple disease-modifying medicines in neurological medicine.
Funding: Efficacy and Mechanism Evaluation (EME) Programme, an MRC and NIHR partnership, UK Multiple Sclerosis Society, and US National Multiple Sclerosis Society.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Feast or famine in multiple sclerosis therapeutics.Lancet Neurol. 2020 Mar;19(3):196-197. doi: 10.1016/S1474-4422(19)30487-9. Epub 2020 Jan 22. Lancet Neurol. 2020. PMID: 31981515 No abstract available.
-
MS-SMART study: systematic sampling bias concerns - Authors' reply.Lancet Neurol. 2020 Jun;19(6):479-480. doi: 10.1016/S1474-4422(20)30149-6. Epub 2020 May 26. Lancet Neurol. 2020. PMID: 32470412 No abstract available.
-
MS-SMART study: systematic sampling bias concerns.Lancet Neurol. 2020 Jun;19(6):479. doi: 10.1016/S1474-4422(20)30152-6. Epub 2020 May 26. Lancet Neurol. 2020. PMID: 32470413 No abstract available.
References
-
- Ontaneda D, Thompson AJ, Fox RJ, Cohen JA. Progressive multiple sclerosis: prospects for disease therapy, repair, and restoration of function. Lancet. 2017;389:1357–1366. - PubMed
-
- Kappos L, Bar-Or A, Cree BAC. Siponimod versus placebo in secondary progressive multiple sclerosis (EXPAND): a double-blind, randomised, phase 3 study. Lancet. 2018;391:1263–1273. - PubMed
-
- Montalban X, Hauser SL, Kappos L. Ocrelizumab versus placebo in primary progressive multiple sclerosis. N Engl J Med. 2017;376:209–220. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
