

Cause-specific mortality of children younger than 5 years in communities receiving biannual mass azithromycin treatment in Niger: verbal autopsy results from a cluster-randomised controlled trial
- PMID: 31981558
- PMCID: PMC7025321
- DOI: 10.1016/S2214-109X(19)30540-6
Cause-specific mortality of children younger than 5 years in communities receiving biannual mass azithromycin treatment in Niger: verbal autopsy results from a cluster-randomised controlled trial
Abstract
Background: The Macrolides Oraux pour Réduire les Décès avec un Oeil sur la Résistance (MORDOR) trial found that biannual mass distribution of azithromycin to children younger than 5 years in Niger reduced the primary outcome of all-cause mortality by 18%. We aimed to determine the causes of mortality among deceased children using verbal autopsy.
Methods: In this 2-year cluster-randomised controlled trial, 594 community clusters in Niger were randomly allocated (1:1 ratio) to receive biannual mass distributions of either oral azithromycin (approximately 20 mg per kg of bodyweight) or placebo targeted to children aged 1-59 months. Participants, study investigators, and field workers were masked to treatment allocation. Between Nov 23, 2014, and July 31, 2017, 3615 child deaths were recorded by use of biannual house-to-house censuses, and verbal autopsies were done between May 26, 2015, and May 17, 2018, to identify cause of death. Cause-specific mortality, as assessed by verbal autopsy, was a prespecified secondary outcome. This trial is completed and is registered with ClinicalTrials.gov, NCT02047981.
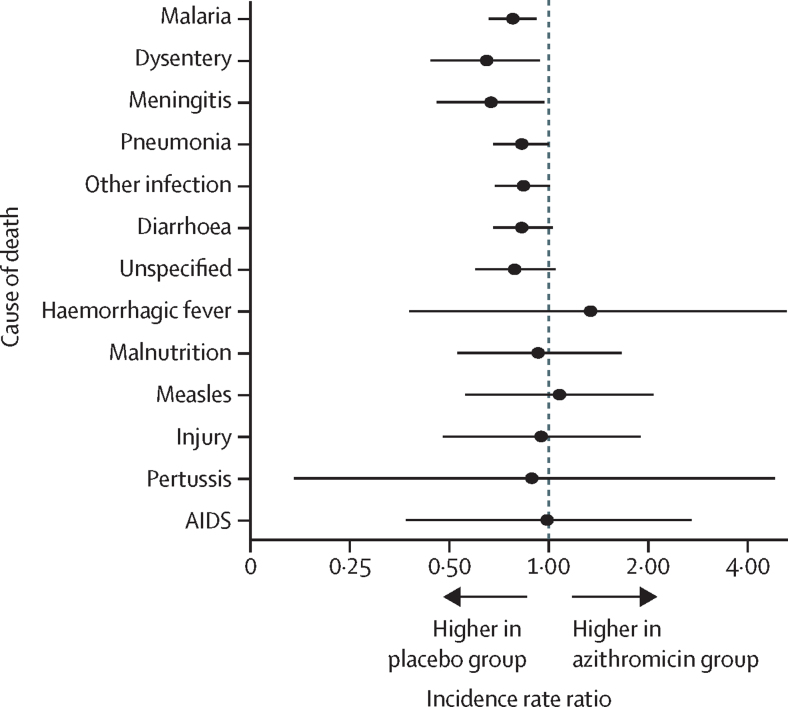
Findings: Between Nov 23, 2014, and July 31, 2017, 303 communities (n=40 375 children at baseline) in Niger received mass azithromycin and 291 communities (n=35 747 children at baseline) received placebo. Treatment coverage was 90·3% (SD 10·6) in the azithromycin group and 90·4% (10·1) in the placebo group. No communities were lost to follow-up. In total, 1727 child deaths in the azithromycin group and 1888 child deaths in the placebo group were reported from the population censuses. Of these, the cause of death for 1566 (90·7%) children in the azithromycin group and 1735 (91·9%) children in the placebo group were ascertained by verbal autopsy interviews. In the azithromycin group, 437 (27·9%) deaths were due to malaria, 252 (16·1%) deaths were due to pneumonia, and 234 (14·9%) deaths were due to diarrhoea. In the placebo group, 493 (28·4%) deaths were due to malaria, 275 (15·9%) deaths were due to pneumonia, and 251 (14·5%) deaths were due to diarrhoea. Relative to communities that received placebo, child mortality in communities that received azithromycin was lower for malaria (incidence rate ratio 0·78, 95% CI 0·66-0·92; p=0·0029), dysentery (0·65, 0·44-0·94; p=0·025), meningitis (0·67, 0·46-0·97; p=0·036), and pneumonia (0·83, 0·68-1·00; p=0·051). The distribution of causes of death did not differ significantly between the two study groups (p=0·98).
Interpretation: Mass azithromycin distribution resulted in approximately a third fewer deaths in children aged 1-59 months due to meningitis and dysentery, and a fifth fewer deaths due to malaria and pneumonia. The lack of difference in the distribution of causes of death between the azithromycin and placebo groups could be attributable to the broad spectrum of azithromycin activity and the study setting, in which most childhood deaths were due to infections.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures

Comment in
-
Azithromycin for child survival: digging without getting too dirty into the differential effect on cause-specific mortality.Lancet Glob Health. 2020 Feb;8(2):e169-e170. doi: 10.1016/S2214-109X(19)30558-3. Lancet Glob Health. 2020. PMID: 31981547 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
