

Financial Incentives for Smoking Cessation in Hospitalized Patients: A Randomized Clinical Trial
- PMID: 31982494
- PMCID: PMC7293955
- DOI: 10.1016/j.amjmed.2019.12.025
Financial Incentives for Smoking Cessation in Hospitalized Patients: A Randomized Clinical Trial
Abstract
Background: Financial incentives for smoking cessation and use of evidence-based therapy may increase quitting rates and reduce health and economic disparities.
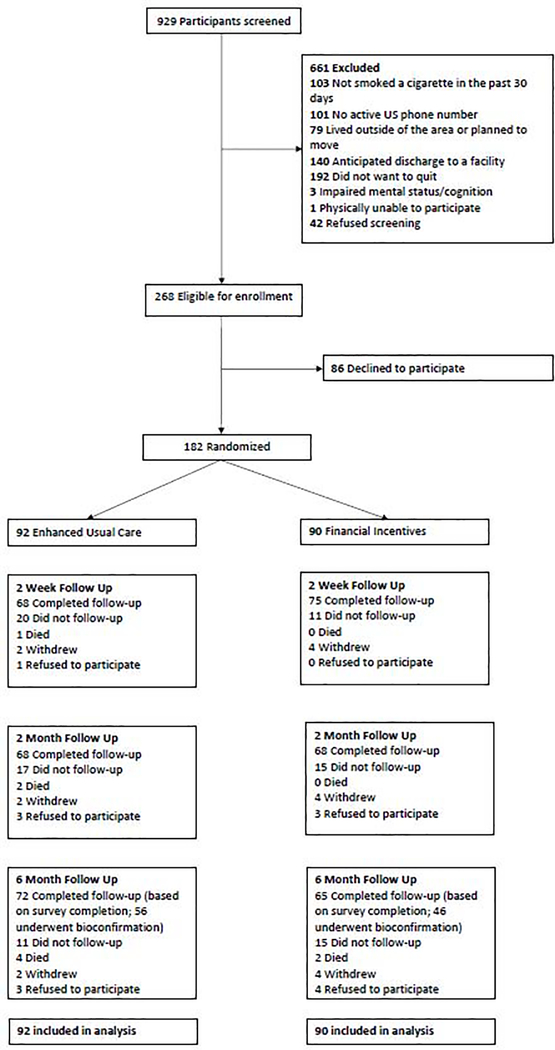
Methods: We randomized a low-income population of 182 hospitalized patients (mean age 58 years, 45% with high school education or less) to enhanced usual care, which included hospital-directed cessation care and Quitline referral or enhanced usual care plus financial incentives. All patients received enhanced usual care, while participants randomized to the financial incentives group were also eligible to receive up to $550 for participation in Quitline counseling ($50), participation in a community-based cessation program ($50), use of pharmacotherapy ($50), and biochemically confirmed smoking cessation at 2 months ($150) and 6 months ($250). Primary outcome was biochemically confirmed smoking cessation at 6 months after hospital discharge.
Results: Total mean payment was $84 (standard deviation [SD] = $133) in the incentive group. The 6-month rate of biochemically confirmed smoking cessation was 19.6% in the incentive group and 8.9% in the enhanced usual care group (odds ratio [OR] 2.56; 95% confidence interval [CI] 0.84 to 7.83, P = 0.10). Participants in the incentive group had higher rates of nicotine replacement therapy use (57.3% vs 31.3%, P = 0.002). Financial incentives did not improve subjective social status but did increase financial stress.
Conclusions: Rates of bioconfirmed smoking cessation were higher among hospitalized patients randomized to financial incentives compared to usual care alone, but the difference was not significant. Considering the frequency of low payouts and the importance of assistance for successful quitting, future studies should explore the effectiveness of financial incentives sufficiently large to overcome barriers to evidence-based therapy.
Keywords: FIESTA; Financial Incentives; Manhattan VA Hospital; Smoking cessation; Veterans.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Competing Interests
N/A
Figures
References
-
- National Center for Chronic Disease P, Health Promotion Office on S, Health. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta (GA): Centers for Disease Control and Prevention (US); 2014.
-
- Jha P, Ramasundarahettige C, Landsman V, et al. 21st-century hazards of smoking and benefits of cessation in the United States. N Engl J Med. 2013;368(4):341–350. - PubMed
-
- Critchley JA, Capewell S. Mortality risk reduction associated with smoking cessation in patients with coronary heart disease: a systematic review. JAMA. 2003;290(1):86–97. - PubMed
-
- Mills E, Eyawo O, Lockhart I, Kelly S, Wu P, Ebbert JO. Smoking cessation reduces postoperative complications: a systematic review and meta-analysis. Am J Med. 2011;124(2):144–154 e148. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
