

Sleep, Growth, and Puberty After 2 Years of Prolonged-Release Melatonin in Children With Autism Spectrum Disorder
- PMID: 31982581
- PMCID: PMC8084705
- DOI: 10.1016/j.jaac.2019.12.007
Sleep, Growth, and Puberty After 2 Years of Prolonged-Release Melatonin in Children With Autism Spectrum Disorder
Abstract
Objective: A recent 3-month double-blind, placebo-controlled study demonstrated efficacy and safety of pediatric prolonged-release melatonin (PedPRM) for insomnia in children with autism spectrum disorder. This study examined the long-term effects of PedPRM treatment on sleep, growth, body mass index, and pubertal development.
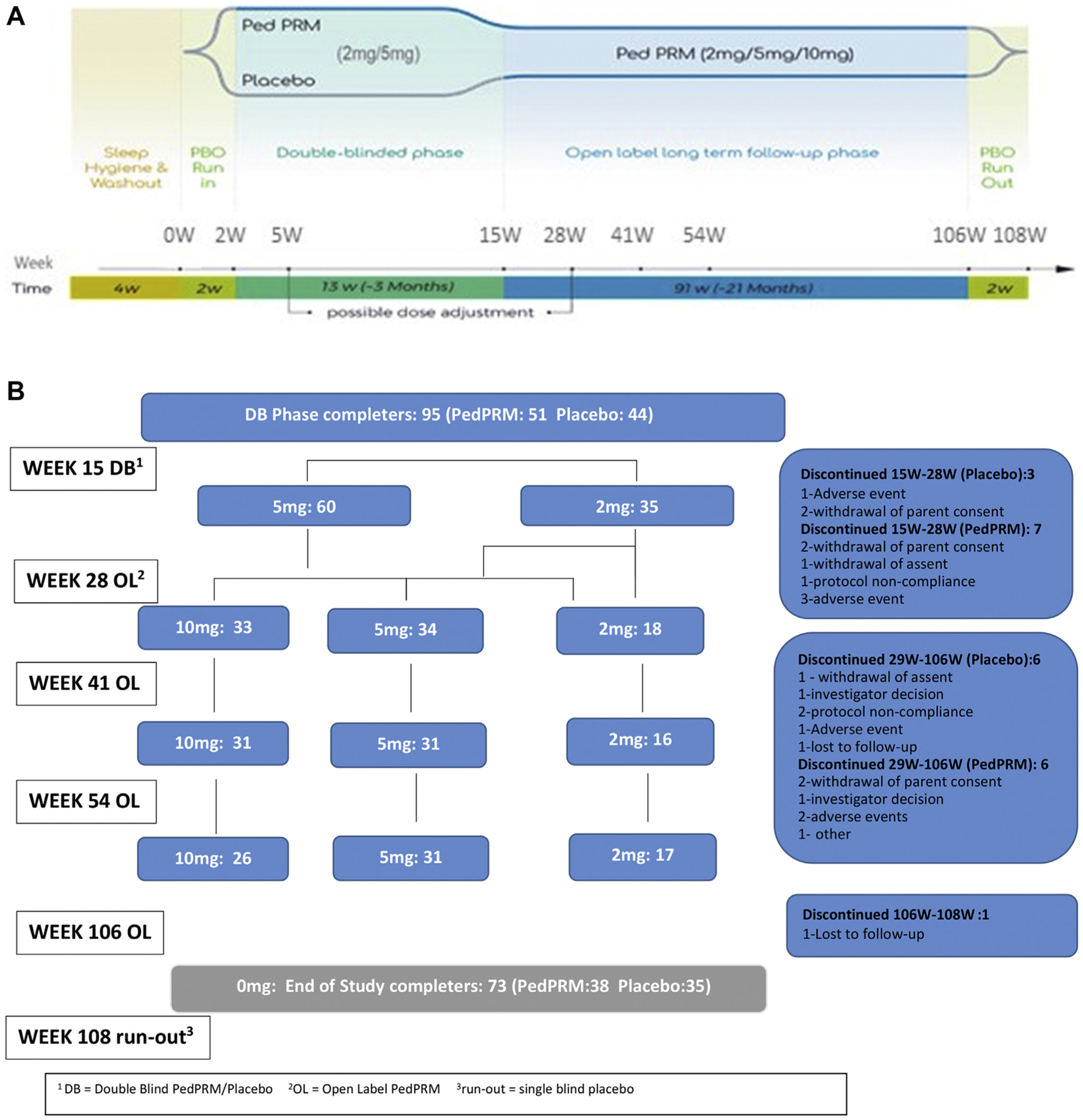
Method: Eighty children and adolescents (2-17.5 years of age; 96% with autism spectrum disorder) who completed the double-blind, placebo-controlled trial were given 2 mg, 5 mg, or 10 mg PedPRM nightly up to 104 weeks, followed by a 2-week placebo period to assess withdrawal effects.
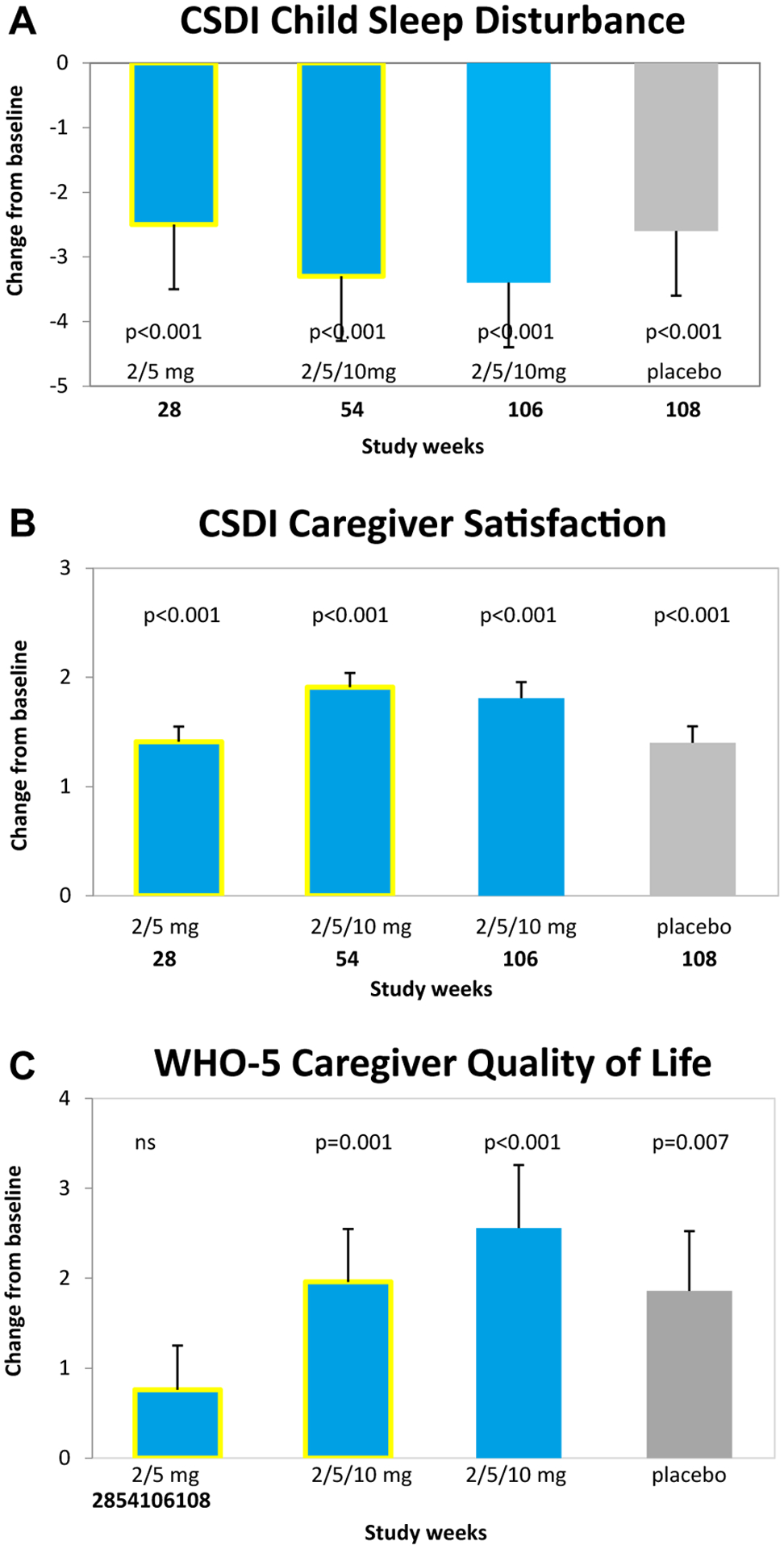
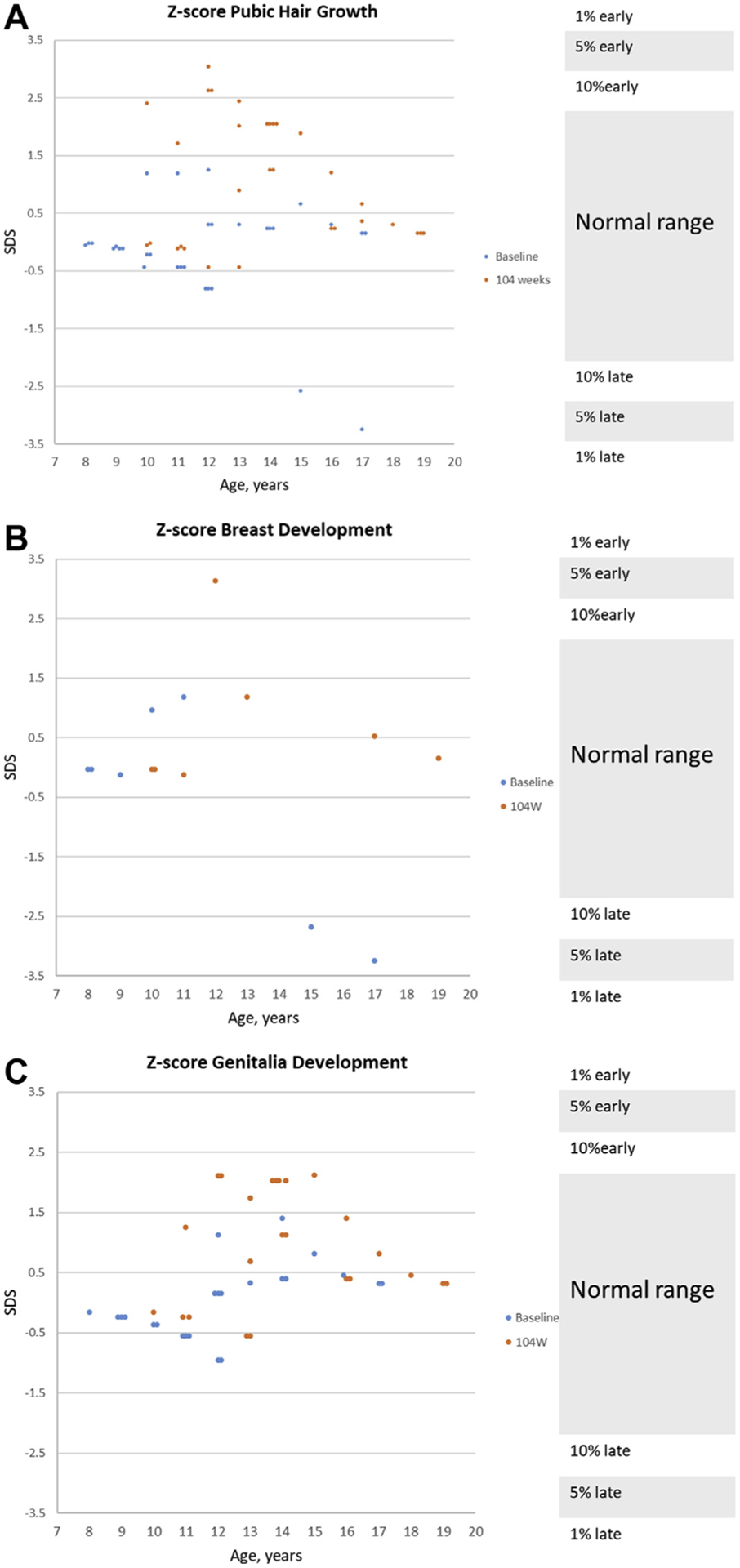
Results: Improvements in child sleep disturbance and caregiver satisfaction with child sleep patterns, quality of sleep, and quality of life were maintained throughout the 104-week treatment period (p < .001 versus baseline for all). During the 2-week withdrawal placebo period, measures declined compared with the treatment period but were still improved compared with baseline. PedPRM was generally safe; the most frequent treatment-related adverse events were fatigue (6.3%), somnolence (6.3%), and mood swings (4.2%). Changes in mean weight, height, body mass index, and pubertal status (Tanner staging done by a physician) were within normal ranges for age with no evidence of delay in body mass index or pubertal development.
Conclusion: Nightly PedPRM at optimal dose (2, 5, or 10 mg nightly) is safe and effective for long-term treatment in children and adolescents with autism spectrum disorder and insomnia. There were no observed detrimental effects on children's growth and pubertal development and no withdrawal or safety issues related to the use or discontinuation of the drug.
Clinical trial registration information: Efficacy and Safety of Circadin in the Treatment of Sleep Disturbances in Children With Neurodevelopment Disabilities; https://clinicaltrials.gov/; NCT01906866.
Keywords: autism; melatonin; sleep.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Cuomo BM, Vaz S, Lee EAL, Thompson C, Rogerson JM, Falkmer T. Effectiveness of sleep-based interventions for children with autism spectrum disorder: a meta-synthesis. Pharmacotherapy. 2017;37:555–578. - PubMed
-
- Taira M, Takase M, Sasaki H. Sleep disorder in children with autism. Psychiatry Clin Neurosci. 1998;52:182–183. - PubMed
-
- Elrod MG, Hood BS. Sleep differences among children with autism spectrum disorders and typically developing peers: a meta-analysis. J Dev Behav Pediatr. 2015;36:166–177. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
