

Three-dimensional biventricular strains in pulmonary arterial hypertension patients using hyperelastic warping
- PMID: 31982668
- PMCID: PMC7198336
- DOI: 10.1016/j.cmpb.2020.105345
Three-dimensional biventricular strains in pulmonary arterial hypertension patients using hyperelastic warping
Abstract
Background and objective: Evaluation of biventricular function is an essential component of clinical management in pulmonary arterial hypertension (PAH). This study aims to examine the utility of biventricular strains derived from a model-to-image registration technique in PAH patients in comparison to age- and gender-matched normal controls.
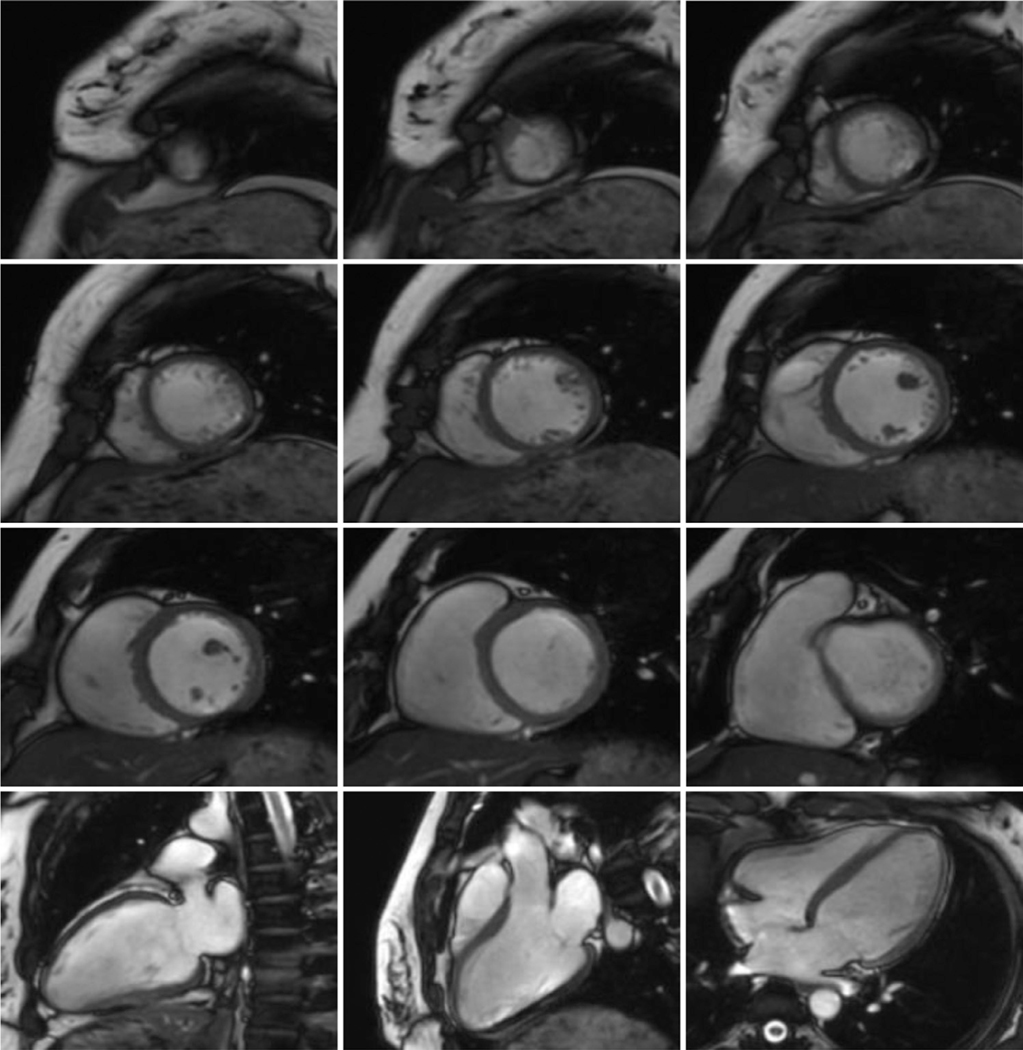
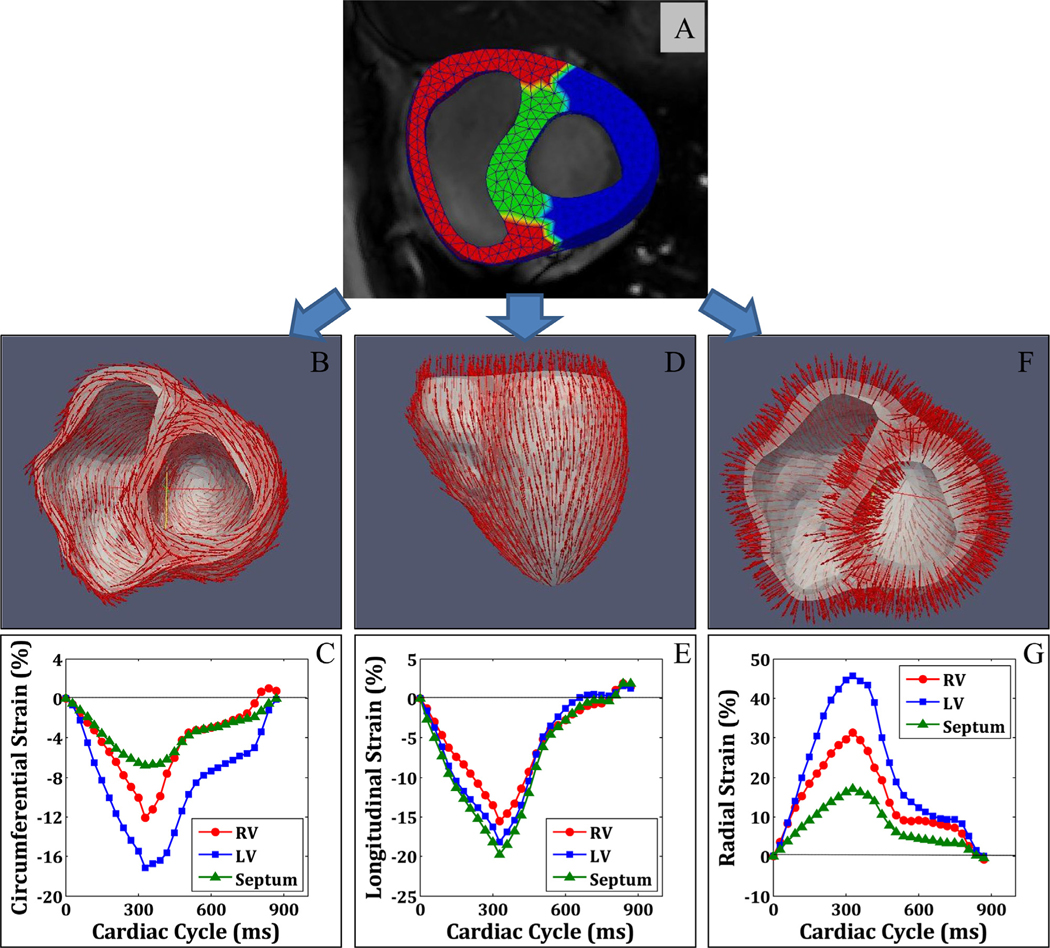
Methods: A three-dimensional (3D) model was reconstructed from cine short- and long-axis cardiac magnetic resonance (CMR) images and subsequently partitioned into right ventricle (RV), left ventricle (LV) and septum. The hyperelastic warping method was used to register the meshed biventricular finite element model throughout the cardiac cycle and obtain the corresponding biventricular circumferential, longitudinal and radial strains.
Results: Intra- and inter-observer reproducibility of biventricular strains was excellent with all intra-class correlation coefficients > 0.84. 3D biventricular longitudinal, circumferential and radial strains for RV, LV and septum were significantly decreased in PAH patients compared with controls. Receiver operating characteristic (ROC) analysis showed that the 3D biventricular strains were better early markers (Area under the ROC curve = 0.96 for RV longitudinal strain) of ventricular dysfunction than conventional parameters such as two-dimensional strains and ejection fraction.
Conclusions: Our highly reproducible methodology holds potential for extending CMR imaging to characterize 3D biventricular strains, eventually leading to deeper understanding of biventricular mechanics in PAH.
Keywords: Biventricular strain; Cardiac magnetic resonance; Hyperelastic warping; Pulmonary arterial hypertension.
Copyright © 2020 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors have no conflicts of interest, financial or otherwise.
Figures




References
-
- Callan P, Clark AL, Right heart catheterisation: indications and interpretation, Heart 102 (2016) 1–11. - PubMed
-
- Van Der Zwaan HB, Geleijnse ML, McGhie JS, Boersma E, Helbing WA, Meijboom FJ, Roos-Hesselink JW, Right ventricular quantification in clinical practice: two-dimensional vs. three-dimensional echocardiography compared with cardiac magnetic resonance imaging, Eur. J. Echocardiogr 12 (2011) 656–664. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
