

Oral contraceptive use, bone mineral density, and bone turnover markers over 12 months in college-aged females
- PMID: 31983034
- PMCID: PMC10317246
- DOI: 10.1007/s00774-019-01081-1
Oral contraceptive use, bone mineral density, and bone turnover markers over 12 months in college-aged females
Abstract
Introduction: The purpose of this study was to compare bone mineral density (BMD) and bone turnover markers between combined oral contraceptive (COC) and non-COC users over 12 months.
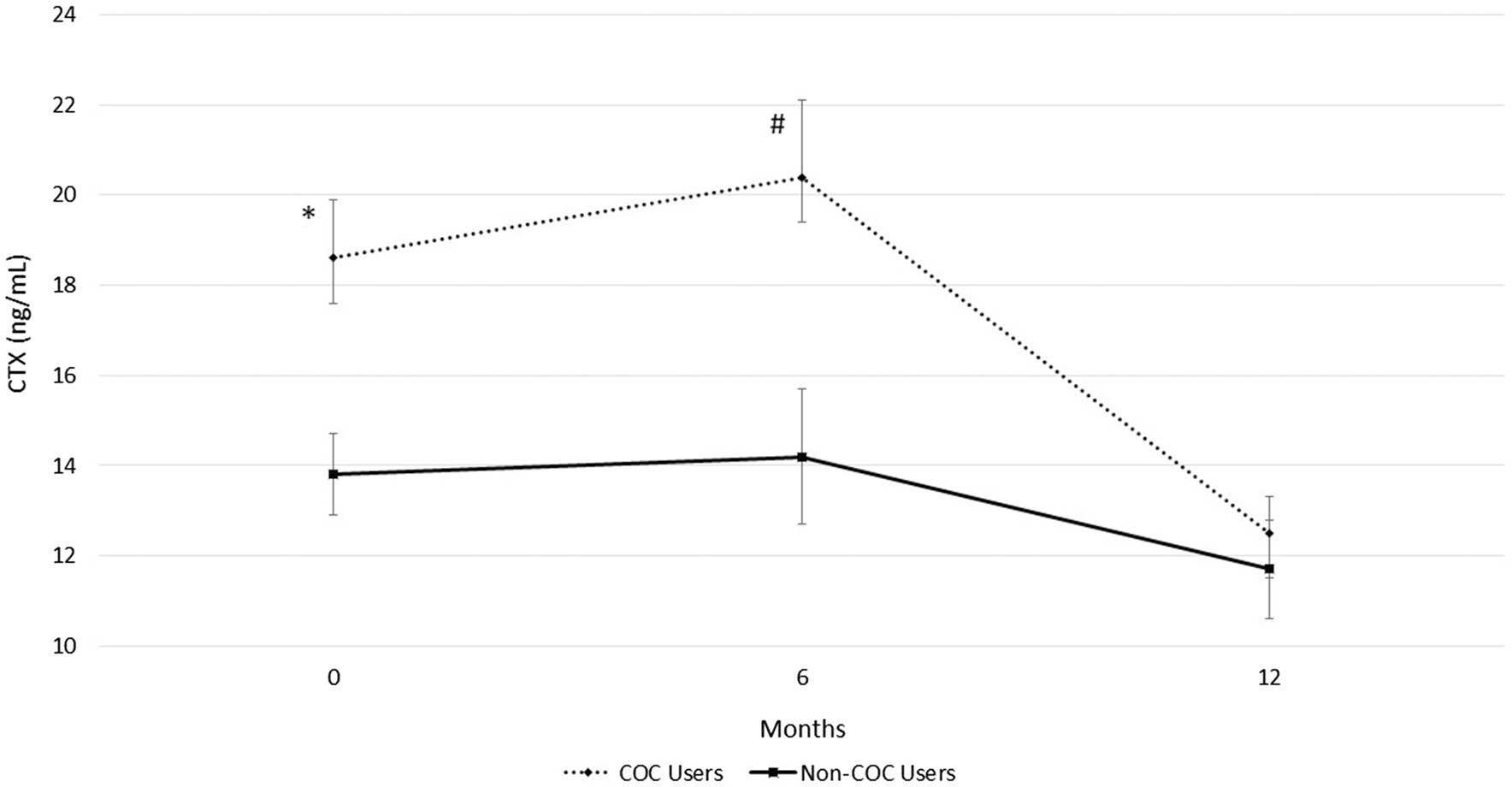
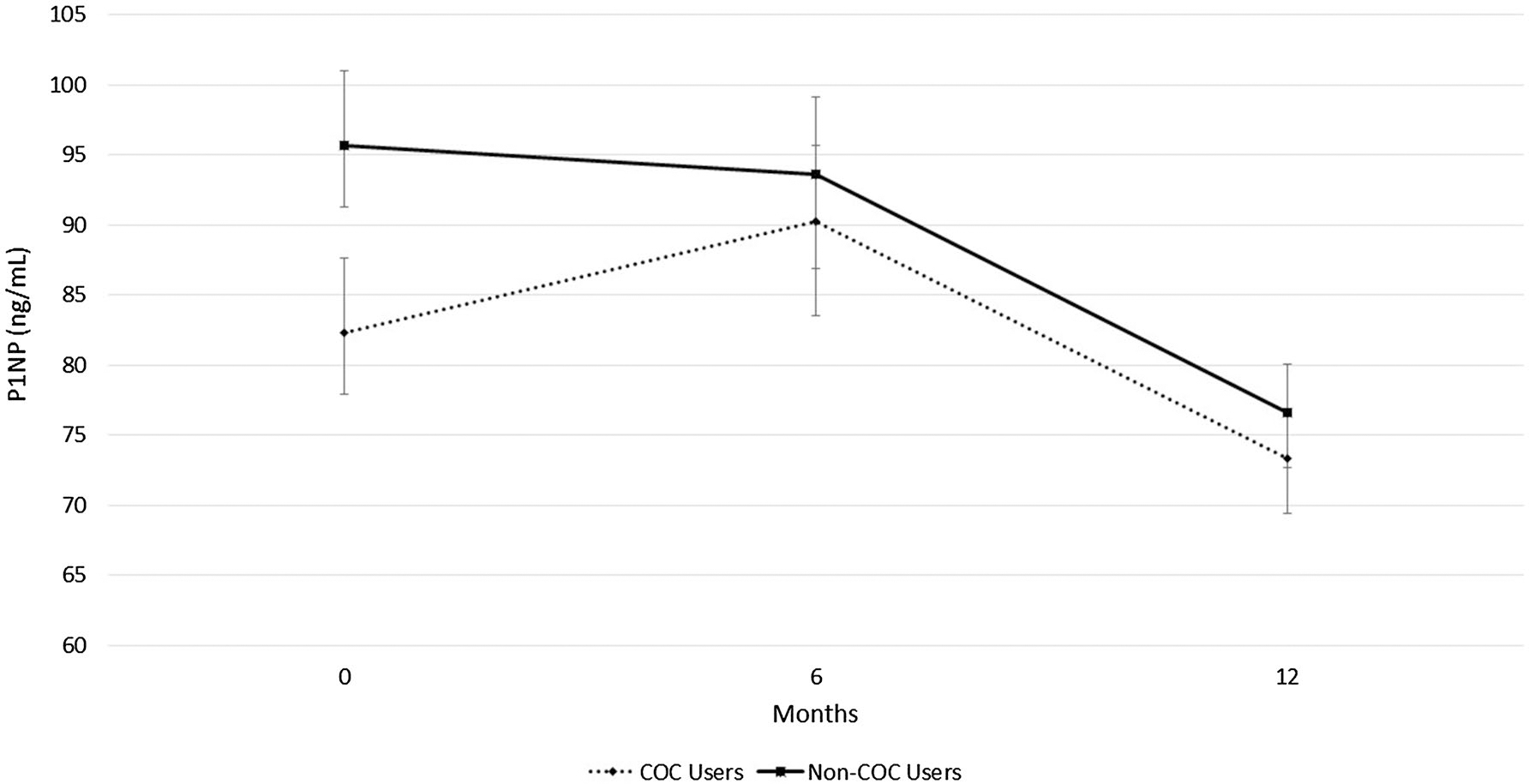
Materials and methods: COC users (n = 34, age = 19.2 ± 0.5) and non-COC users (n = 28, age = 19.3 ± 0.6) provided serum at baseline, 6 months, and 12 months. C-terminal telopepetides (CTX) and pro-collagen type 1 N-terminal propeptides (P1NP) were determined using ELISA. BMD was measured at the three time points using dual-energy x-ray absorptiometry (DXA).
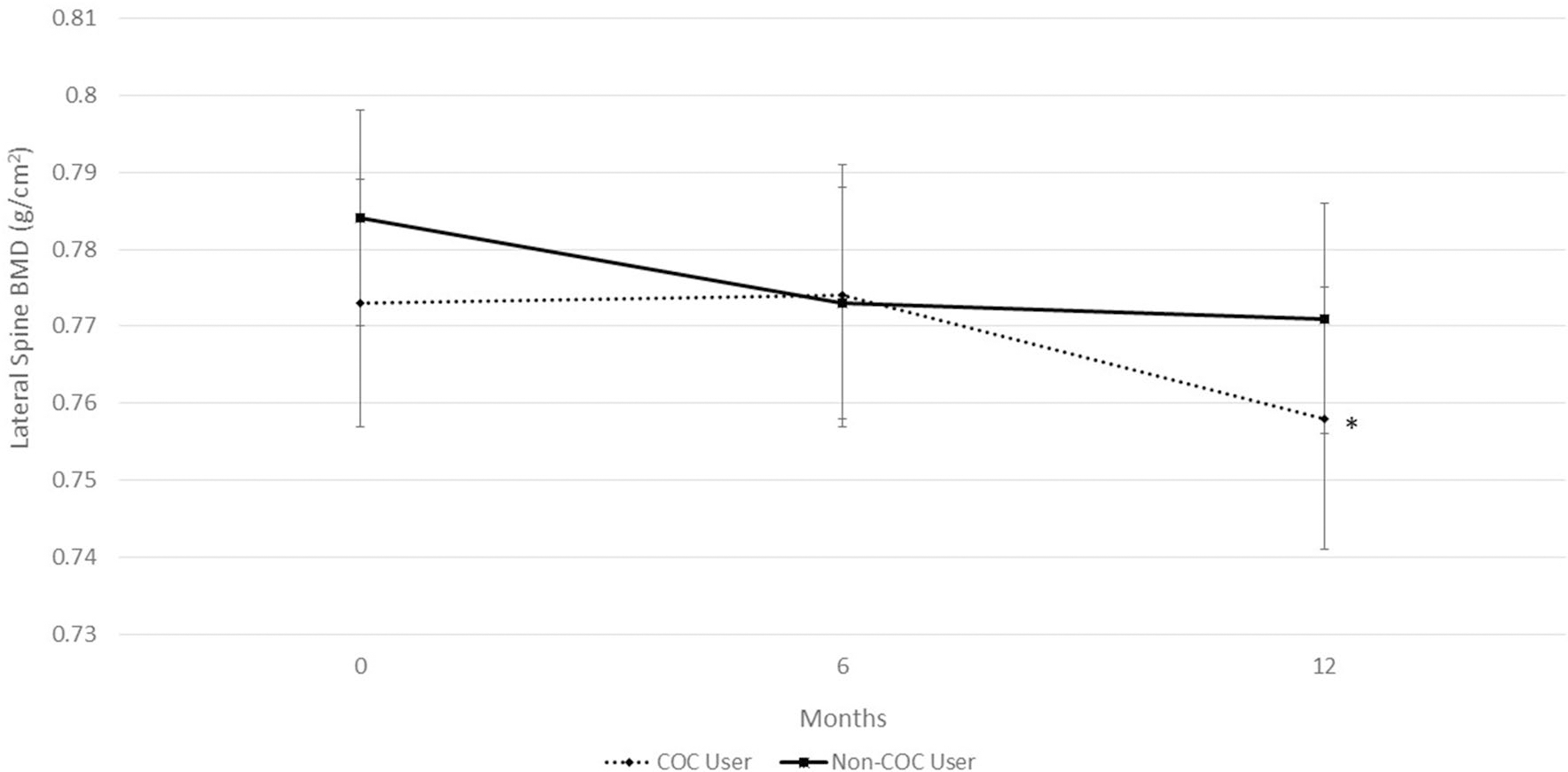
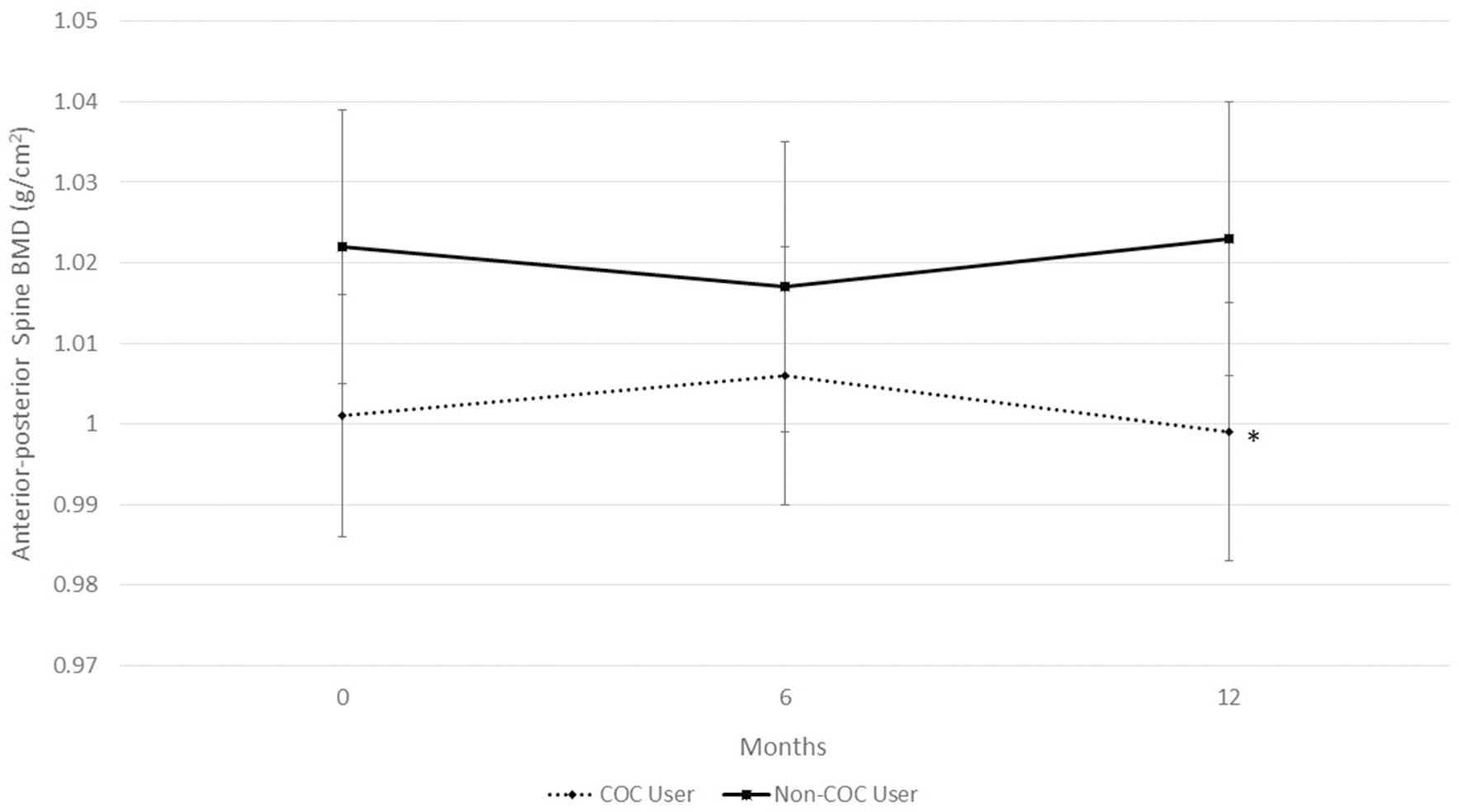
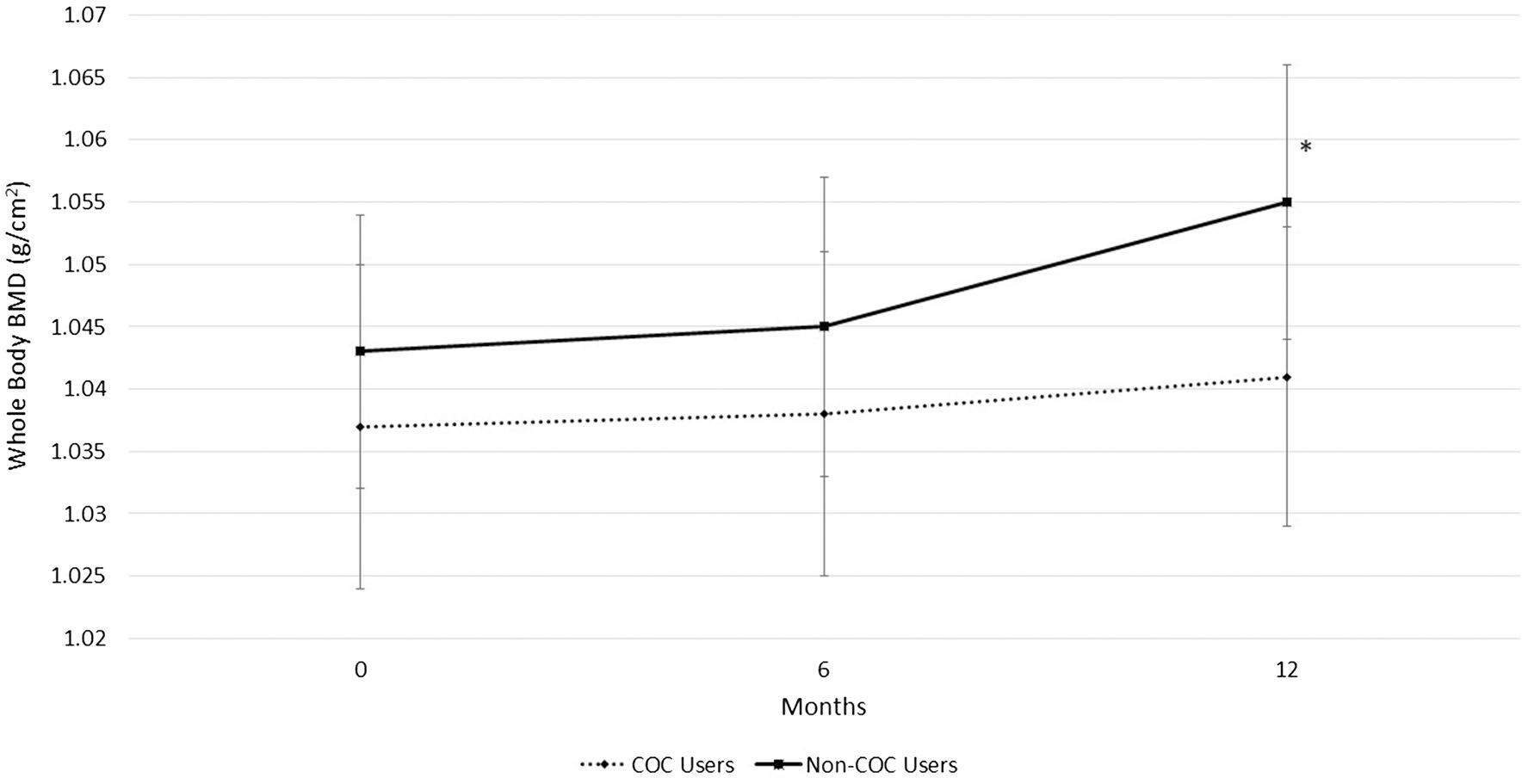
Results: COC users had greater CTX than non-COC users at baseline (18.6 ± 8.2 vs. 13.8 ± 5.3 ng/mL, P = 0.021) and 6 months (20.4 ± 10.3 vs. 14.2 ± 8.5 ng/mL, P = 0.018). Controlling for lean mass, groups were similar in BMD. Over 12 months, non-COC users maintained BMD at the spine, while the COC users declined 2.2% in lateral spine BMD (0.773 ± 0.014 to 0.756 ± 0.014 g/cm2, P = 0.03) and 0.7% in anterior-posterior spine BMD (1.005 ± 0.015 to 0.998 ± 0.015 g/cm2, P = 0.069). Non-COC users increased in BMD of the whole body over 12 months (P < 0.001) while COC users had no change. Women who began COCs within 4 years after menarche had lower BMD at the hip and whole body. Women taking very low dose COCs (20 mcg ethinyl estradiol, EE) significantly declined in CTX, P1NP, and lateral spine BMD in comparison to participants using low dose COCs (30/35 mcg EE).
Conclusion: College-aged women who did not use COCs increased BMD of the whole body, while COC users had elevated bone turnover, declines in spinal BMD, and lack of bone acquisition of the whole body over 12 months. Young females who initiate COC use early after menarche may experience skeletal detriments.
Keywords: CTX; Menarche; P1NP; Peak bone mass; Premenopausal.
Conflict of interest statement
Compliance with ethical standards
Figures
References
-
- United Nations, Department of Economic and Social Affairs, Population Division (2015) Trends in Contraceptive Use Worldwide 2015 (ST/ESA/SER.A/349)
-
- Abma JC, Martinez GM (2017) Sexual activity and contraceptive use among teenagers in the United States, 2011–2015. Natl Health Stat Report, pp 1–23 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
