

Risk of hypoglycaemia with insulin degludec versus insulin glargine U300 in insulin-treated patients with type 2 diabetes: the randomised, head-to-head CONCLUDE trial
- PMID: 31984443
- PMCID: PMC7054369
- DOI: 10.1007/s00125-019-05080-9
Risk of hypoglycaemia with insulin degludec versus insulin glargine U300 in insulin-treated patients with type 2 diabetes: the randomised, head-to-head CONCLUDE trial
Abstract
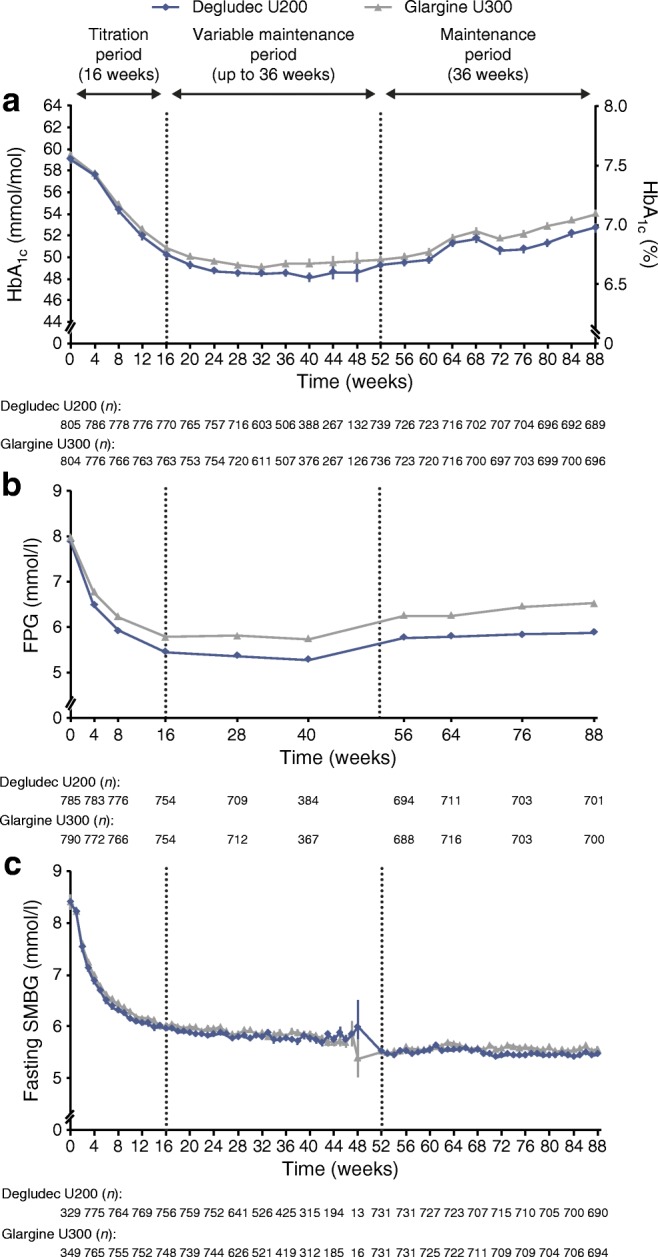
Aims/hypothesis: A head-to-head randomised trial was conducted to evaluate hypoglycaemia safety with insulin degludec 200 U/ml (degludec U200) and insulin glargine 300 U/ml (glargine U300) in individuals with type 2 diabetes treated with basal insulin.
Methods: This randomised (1:1), open-label, treat-to-target, multinational trial included individuals with type 2 diabetes, aged ≥18 years with HbA1c ≤80 mmol/mol (9.5%) and BMI ≤45 kg/m2. Participants were previously treated with basal insulin with or without oral glucose-lowering drugs (excluding insulin secretagogues) and had to fulfil at least one predefined criterion for hypoglycaemia risk. Both degludec U200 and glargine U300 were similarly titrated to a fasting blood glucose target of 4.0-5.0 mmol/l. Endpoints were assessed during a 36 week maintenance period and a total treatment period up to 88 weeks. There were three hypoglycaemia endpoints: (1) overall symptomatic hypoglycaemia (either severe, an event requiring third-party assistance, or confirmed by blood glucose [<3.1 mmol/l] with symptoms); (2) nocturnal symptomatic hypoglycaemia (severe or confirmed by blood glucose with symptoms, between 00:01 and 05:59 h); and (3) severe hypoglycaemia. The primary endpoint was the number of overall symptomatic hypoglycaemic events in the maintenance period. Secondary hypoglycaemia endpoints included the number of nocturnal symptomatic events and number of severe hypoglycaemic events during the maintenance period.
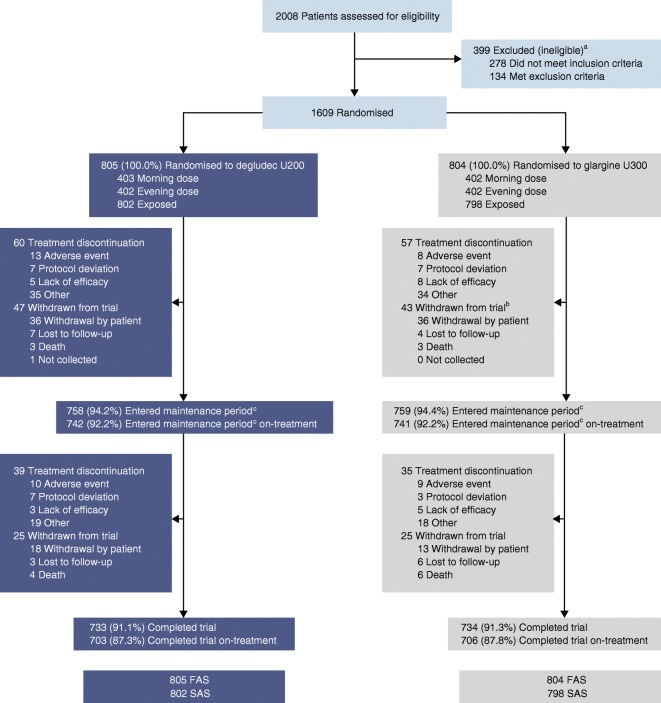
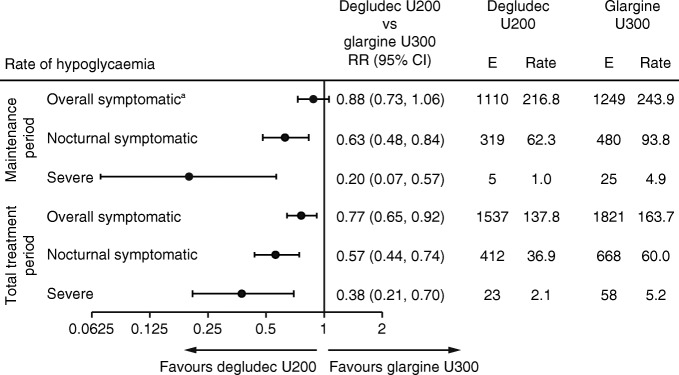
Results: Of the 1609 randomised participants, 733 of 805 (91.1%) in the degludec U200 arm and 734 of 804 (91.3%) in the glargine U300 arm completed the trial (87.3% and 87.8% completed on treatment, respectively). Baseline characteristics were comparable between the two treatment arms. For the primary endpoint, the rate of overall symptomatic hypoglycaemia was not significantly lower with degludec U200 vs glargine U300 (rate ratio [RR] 0.88 [95% CI 0.73, 1.06]). As there was no significant difference between treatments for the primary endpoint, the confirmatory testing procedure for superiority was stopped. The pre-specified confirmatory secondary hypoglycaemia endpoints were analysed using pre-specified statistical models but were now considered exploratory. These endpoints showed a lower rate of nocturnal symptomatic hypoglycaemia (RR 0.63 [95% CI 0.48, 0.84]) and severe hypoglycaemia (RR 0.20 [95% CI 0.07, 0.57]) with degludec U200 vs glargine U300.
Conclusions/interpretation: There was no significant difference in the rate of overall symptomatic hypoglycaemia with degludec U200 vs glargine U300 in the maintenance period. The rates of nocturnal symptomatic and severe hypoglycaemia were nominally significantly lower with degludec U200 during the maintenance period compared with glargine U300.
Trial registration: ClinicalTrials.gov NCT03078478 FUNDING: This trial was funded by Novo Nordisk (Bagsvaerd, Denmark).
Keywords: Clinical science; Hypoglycaemia; Insulin degludec; Insulin glargine; Insulin therapy.
Figures


Comment in
-
How conclusive is the CONCLUDE trial?Diabetologia. 2020 Apr;63(4):692-697. doi: 10.1007/s00125-020-05086-8. Epub 2020 Jan 16. Diabetologia. 2020. PMID: 31950229
References
-
- Leiter LA, Yale J-F, Chiasson J-L, Harris S, Kleinstiver P, Sauriol L. Assessment of the impact of fear of hypoglycemic episodes on glycemic and hypoglycemia management. Can J Diabetes. 2005;29(3):186–192.
-
- Becker RH, Dahmen R, Bergmann K, Lehmann A, Jax T, Heise T. New insulin glargine 300 units ml−1 provides a more even activity profile and prolonged glycemic control at steady state compared with insulin glargine 100 units ml−1. Diabetes Care. 2015;38(4):637–643. doi: 10.2337/dc14-0006. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
