

Quality improvement of intravenous to oral medication conversion using Lean Six Sigma methodologies
- PMID: 31986120
- PMCID: PMC7011893
- DOI: 10.1136/bmjoq-2019-000804
Quality improvement of intravenous to oral medication conversion using Lean Six Sigma methodologies
Abstract
Introduction: Lack of medication conversion from intravenous to oral contributes to increased risk of infection, delayed discharges and higher medication costs. At our institution, intravenous to oral medication conversion rate was 76% with missed opportunity for conversion of 37%. The goal of the project was to reduce the percent of missed opportunities for intravenous to oral conversion for applicable medications.
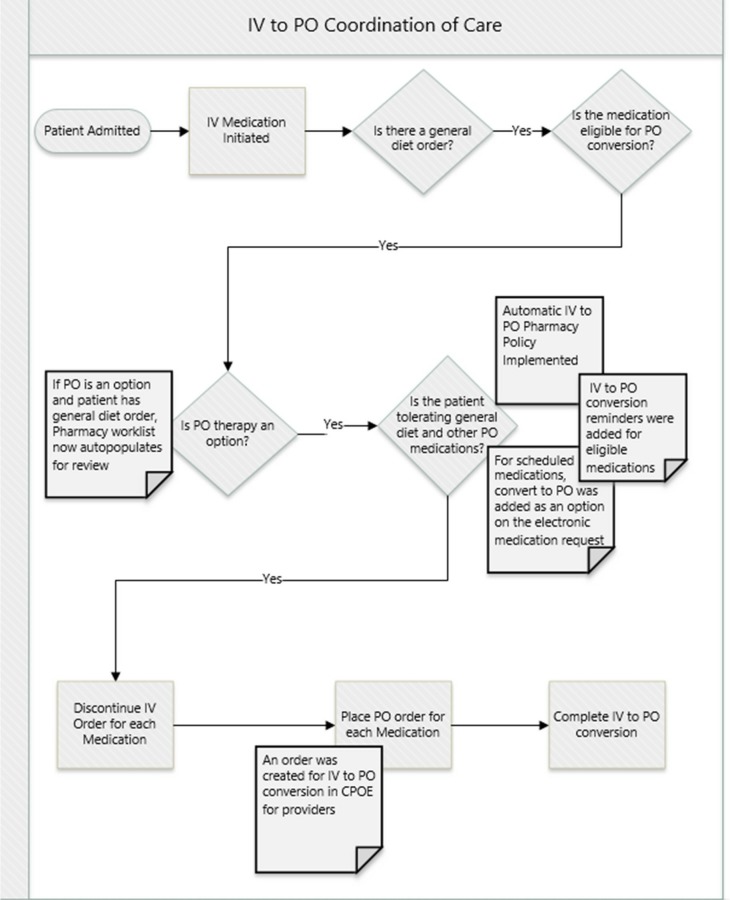
Methods: A pharmacy-driven intravenous to oral policy and procedure was implemented. To identify potential opportunities, a patient worklist of applicable intravenous to oral medications was created for pharmacy review in real time. An intravenous to oral conversion order was implemented in the computerised provider order entry. 'Convert to oral' was added as an option in the electronic medication request and highlighted reminders were added to the electronic medication administration record for eligible medications.
Results: After improvements, the missed opportunity rate for intravenous to oral conversion decreased from 37% (19/51) to 21% (24/113) (p=0.04, two-proportion test), a 43% improvement. The trend in intravenous to oral conversion rate increased from 76% (39/51) to 85% (171/201) and severity adjusted length of stay was reduced from 8.1 days to 6.4 days post improvements (p<0.001, t-test).
Keywords: Six Sigma; antibiotic management; electronic prescribing; healthcare quality improvement; patient discharge.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



Similar articles
-
Use of clinical decision support to identify i.v.-to-oral conversion opportunities and cost savings.Am J Health Syst Pharm. 2018 Dec 1;75(23 Supplement 4):S82-S86. doi: 10.2146/ajhp170405. Epub 2018 Sep 10. Am J Health Syst Pharm. 2018. PMID: 30201658
-
The impacts of a pharmacist-managed outpatient clinic and chemotherapy-directed electronic order sets for monitoring oral chemotherapy.J Oncol Pharm Pract. 2017 Dec;23(8):582-590. doi: 10.1177/1078155216672314. Epub 2016 Oct 12. J Oncol Pharm Pract. 2017. PMID: 27733666
-
Conversion from intravenous to oral medications: assessment of a computerized intervention for hospitalized patients.Arch Intern Med. 2003 Nov 24;163(21):2585-9. doi: 10.1001/archinte.163.21.2585. Arch Intern Med. 2003. PMID: 14638558
-
Can Lean Six Sigma be used to reduce medication errors in the health-care sector?Leadersh Health Serv (Bradf Engl). 2018 Oct 1;31(4):426-433. doi: 10.1108/LHS-09-2017-0055. Epub 2018 Jan 30. Leadersh Health Serv (Bradf Engl). 2018. PMID: 30234447 Review.
-
What is new in paediatric medication safety?Arch Dis Child. 2019 Jun;104(6):596-599. doi: 10.1136/archdischild-2018-315175. Epub 2018 Aug 28. Arch Dis Child. 2019. PMID: 30154183 Review.
Cited by
-
Medication Utilisation Program, Quality Improvement and Research Pharmacist-Implementation Strategies and Preliminary Findings.Pharmacy (Basel). 2021 Nov 4;9(4):182. doi: 10.3390/pharmacy9040182. Pharmacy (Basel). 2021. PMID: 34842809 Free PMC article.
-
Antibiotic utilization, sensitivity, and cost in the medical intensive care unit of a tertiary care teaching hospital in Nepal.SAGE Open Med. 2021 Sep 3;9:20503121211043710. doi: 10.1177/20503121211043710. eCollection 2021. SAGE Open Med. 2021. PMID: 34504707 Free PMC article.
-
Assessment of Intravenous versus Oral Antimicrobials in a Large Regional Health Authority.Can J Hosp Pharm. 2022 Spring;75(2):108-112. doi: 10.4212/cjhp.v75i2.3173. Epub 2022 Apr 4. Can J Hosp Pharm. 2022. PMID: 35387377 Free PMC article.
-
A Health Technology Assessment in Maxillofacial Cancer Surgery by Using the Six Sigma Methodology.Int J Environ Res Public Health. 2021 Sep 18;18(18):9846. doi: 10.3390/ijerph18189846. Int J Environ Res Public Health. 2021. PMID: 34574768 Free PMC article.
-
Leveling Up: Evaluation of IV v. PO Linezolid Utilization and Cost after an Antimicrobial Stewardship Program Revision of IV to PO Conversion Criteria within a Healthcare System.Pharmacy (Basel). 2023 Apr 5;11(2):70. doi: 10.3390/pharmacy11020070. Pharmacy (Basel). 2023. PMID: 37104076 Free PMC article.
References
-
- Kuper KM. Intravenous to oral therapy conversion : Competence assessment tools for health-system pharmacies. 4th edn ASHP, 2008: 347–60.
-
- Tejaswini Y, Challa S, Nalla K, et al. . Practice of intravenous to oral conversion of antibiotics and its influence on length of stay at a tertiary care Hospital: a prospective study. J Clin Diag Res 2018;12:FC01–4.
-
- Chandrasekhar D, PokkaVayalil V. Cost minimization analysis on IV to oral conversion of antimicrobial agent by the clinical pharmacist intervention. Clin Epidemiol Glob Health 2019;7:60–5. 10.1016/j.cegh.2018.01.001 - DOI
MeSH terms
Substances
LinkOut - more resources
Full Text Sources