

Factors associated with hemolysis during extracorporeal membrane oxygenation (ECMO)-Comparison of VA- versus VV ECMO
- PMID: 31986168
- PMCID: PMC6984694
- DOI: 10.1371/journal.pone.0227793
Factors associated with hemolysis during extracorporeal membrane oxygenation (ECMO)-Comparison of VA- versus VV ECMO
Abstract
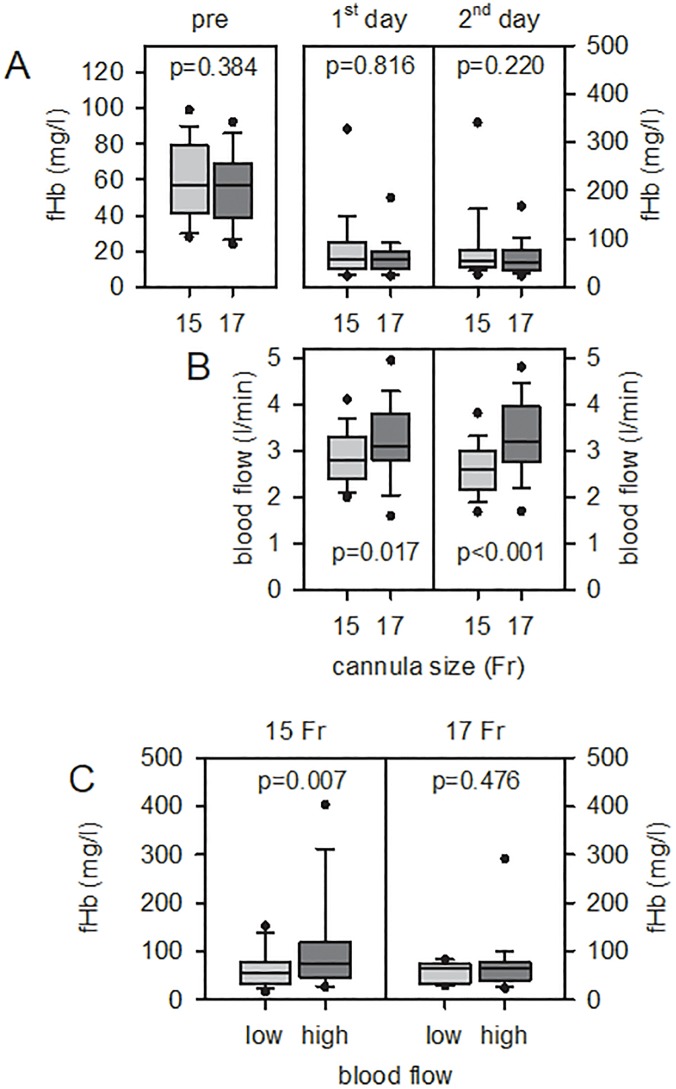
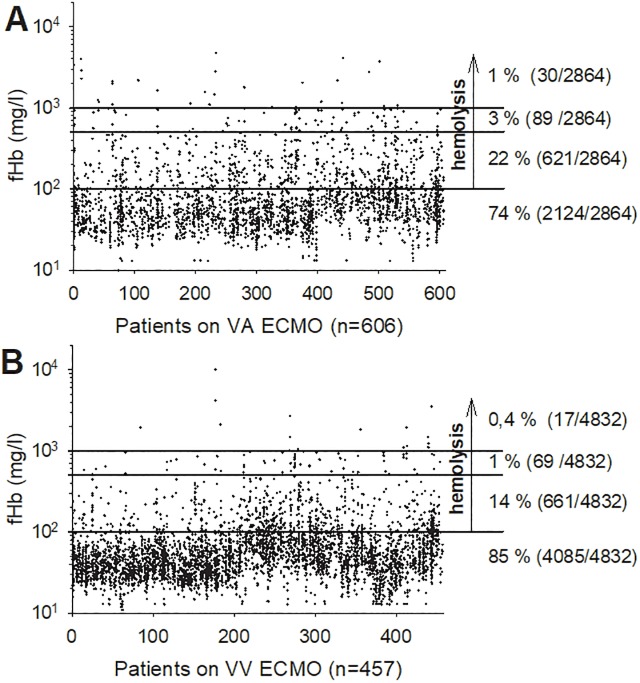
Venovenous (VV) and venoarterial (VA) extracorporeal membrane oxygenation (ECMO) are effective support modalities to treat critically ill patients. ECMO-associated hemolysis remains a serious complication. The aim was to disclose similarities and differences in VA- and VV ECMO-associated hemolysis. This is a retrospective single-center analysis (January 2012 to September 2018) including 1,063 adult consecutive patients (VA, n = 606; VV, n = 457). Severe hemolysis (free plasma hemoglobin, fHb > 500 mg/l) during therapy occurred in 4% (VA) and 2% (VV) (p≤0.001). VV ECMO showed significantly more hemolysis by pump head thrombosis (PHT) compared to VA ECMO (9% vs. 2%; p≤0.001). Pretreatments (ECPR, cardiac surgery) of patients who required VA ECMO caused high fHb pre levels which aggravates the proof of ECMO-induced hemolysis (median (interquartile range), VA: fHb pre: 225.0 (89.3-458.0); VV: fHb pre: 72.0 (42.0-138.0); p≤0.001). The survival rate to discharge from hospital differed depending on ECMO type (40% (VA) vs. 63% (VV); p≤0.001). Hemolysis was dominant in VA ECMO patients, mainly caused by different indications and not by the ECMO support itself. PHT was the most severe form of ECMO-induced hemolysis that occurs in both therapies with low frequency, but more commonly in VV ECMO due to prolonged support time.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Zangrillo A, Landoni G, Biondi-Zoccai G, Greco M, Greco T, Frati G, et al. A meta-analysis of complications and mortality of extracorporeal membrane oxygenation. Critical Care and Resuscitation 2013; 15 (3): 172–178. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
