

Assessing hearing loss in older adults with a single question and person characteristics; Comparison with pure tone audiometry in the Rotterdam Study
- PMID: 31986178
- PMCID: PMC6984733
- DOI: 10.1371/journal.pone.0228349
Assessing hearing loss in older adults with a single question and person characteristics; Comparison with pure tone audiometry in the Rotterdam Study
Abstract
Introduction: Hearing loss (HL) is a frequent problem among the elderly and has been studied in many cohort studies. However, pure tone audiometry-the gold standard-is rather time-consuming and costly for large population-based studies. We have investigated if self-reported hearing loss, using a multiple choice question, can be used to assess HL in absence of pure tone audiometry.
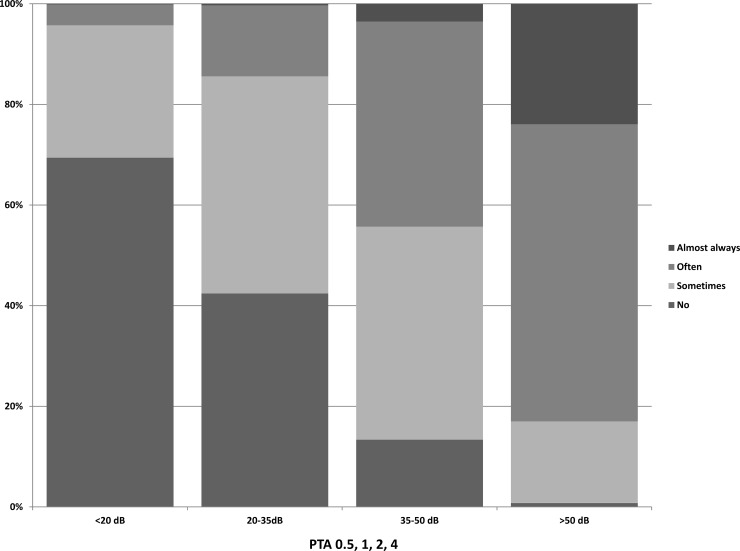
Methods: This study was performed within 4,906 participants of the Rotterdam Study. The question (in Dutch) that was investigated was: 'Do you have any difficulty with your hearing (without hearing aids)?'. The answer options were: 'never', 'sometimes', 'often' and 'daily'. Mild hearing loss or worse was defined as PTA0.5-4(Pure Tone Average 0.5, 1, 2 & 4 kHz) ≥20dBHL and moderate HL or worse as ≥35dBHL. A univariable linear regression model was fitted with the PTA0.5-4 and the answer to the question. Subsequently, sex, age and education were added in a multivariable linear regression model. The ability of the question to classify HL, accounting for sex, age and education, was explored through logistic regression models creating prediction estimates, which were plotted in ROC curves.
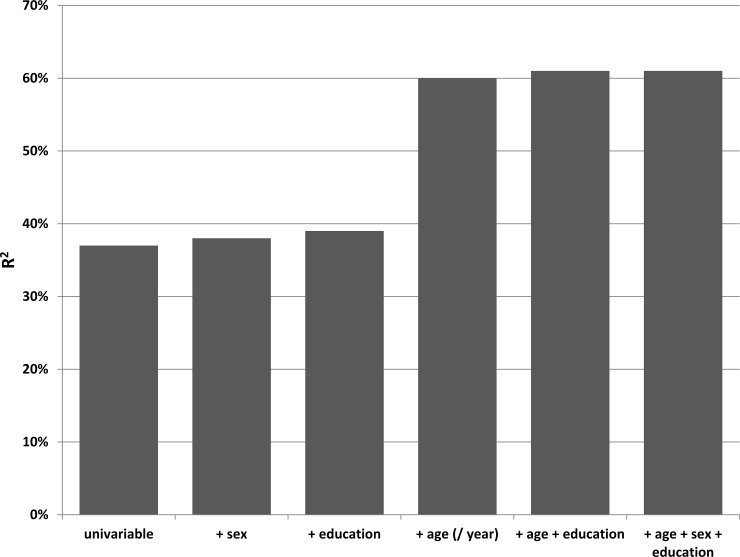
Results: The variance explained (R2) by the univariable regression was 0.37, which increased substantially after adding age (R2 = 0.60). The addition of sex and educational level, however, did not alter the R2 (0.61). The ability of the question to classify hearing loss, reflected in the area under the curve (AUC), was 0.70 (95% CI 0.68, 0.71) for mild hearing loss or worse and 0.86 (95% CI 0.85, 0.87) for moderate hearing loss or worse. The AUC increased substantially when sex, education and age were taken into account (AUC mild HL: 0.73 (95%CI 0.71, 0.75); moderate HL 0.90 (95%CI 0.89, 0.91)).
Conclusion: Self-reported hearing loss using a single question has a good ability to detect hearing loss in older adults, especially when age is accounted for. A single question cannot substitute audiometry, but it can assess hearing loss on a population level with reasonable accuracy.
Conflict of interest statement
The authors have read the journal's policy and the authors of this manuscript have the following competing interests: AG received funding from Cochlear Ltd. BCO and AG also received funding from Heinsius Houbolt fonds. This does not alter our adherence to PLOS ONE policies on sharing data and materials. There are no patents, products in development or marketed products to declare.
Figures
References
-
- Moscicki EK, Elkins EF, Baum HM, McNamara PM. Hearing loss in the elderly: an epidemiologic study of the Framingham Heart Study Cohort. Ear Hear. 1985;6(4):184–90. Epub 1985/07/01. . - PubMed
-
- World Health Organisation W. Grades of hearing impairment [World Health Organisation Web site]. 2015. Available from: http://www.who.int/pbd/deafness/hearing_impairment_grades/en/.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
