

Outcomes and care practices for preterm infants born at less than 33 weeks' gestation: a quality-improvement study
- PMID: 31988152
- PMCID: PMC6989018
- DOI: 10.1503/cmaj.190940
Outcomes and care practices for preterm infants born at less than 33 weeks' gestation: a quality-improvement study
Abstract
Background: Preterm birth is the leading cause of morbidity and mortality in children younger than 5 years. We report the changes in neonatal outcomes and care practices among very preterm infants in Canada over 14 years within a national, collaborative, continuous quality-improvement program.
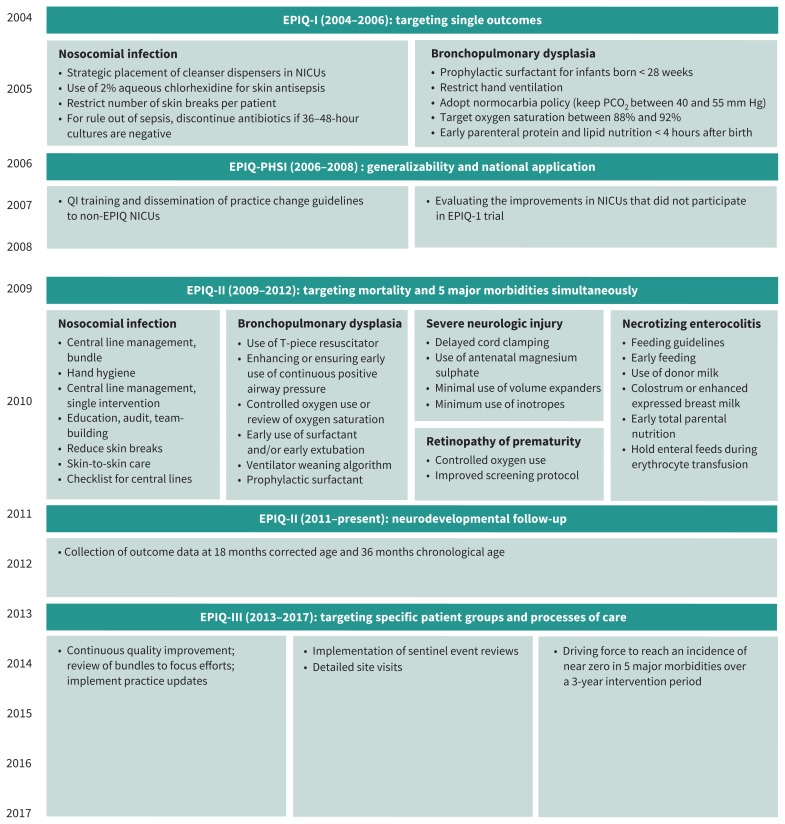
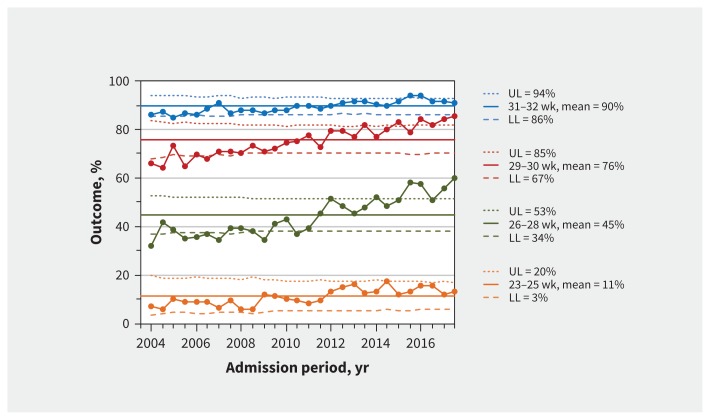
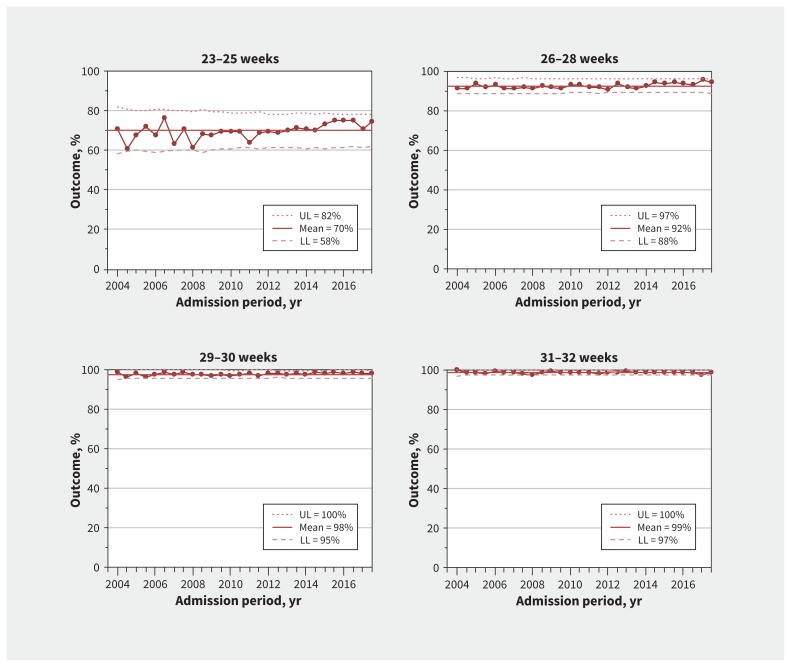
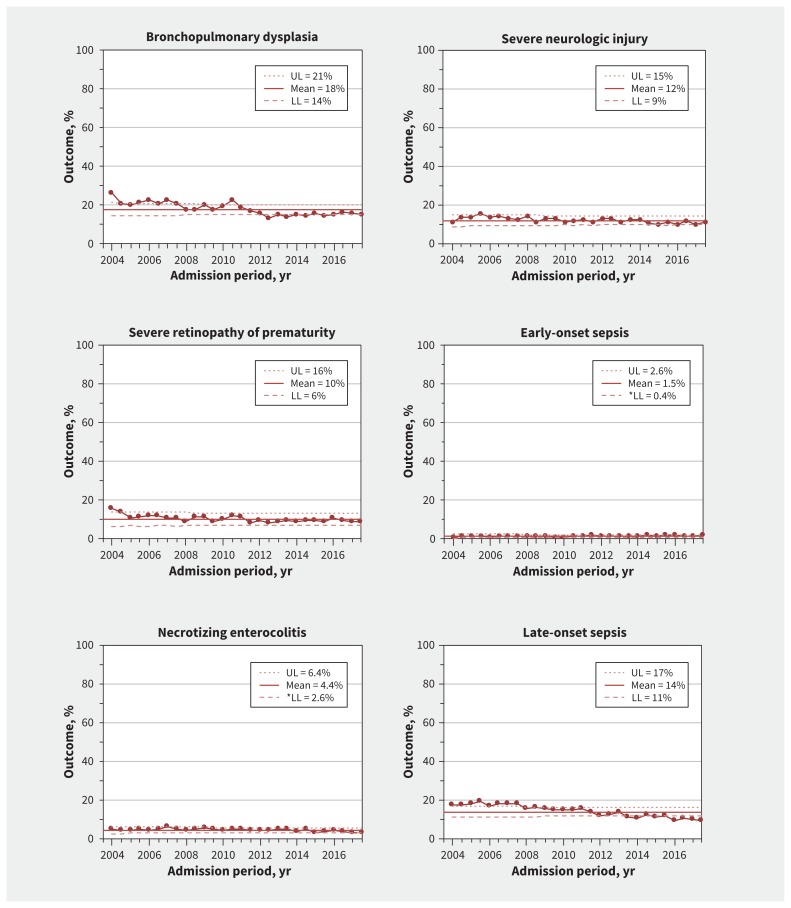
Methods: We retrospectively studied infants born at 23-32 weeks' gestation who were admitted to tertiary neonatal intensive care units that participated in the Evidence-based Practice for Improving Quality program in the Canadian Neonatal Network from 2004 to 2017. The primary outcome was survival without major morbidity during the initial hospital admission. We quantified changes using process-control charts in 6-month intervals to identify special-cause variations, adjusted regression models for yearly changes, and interrupted time series analyses.
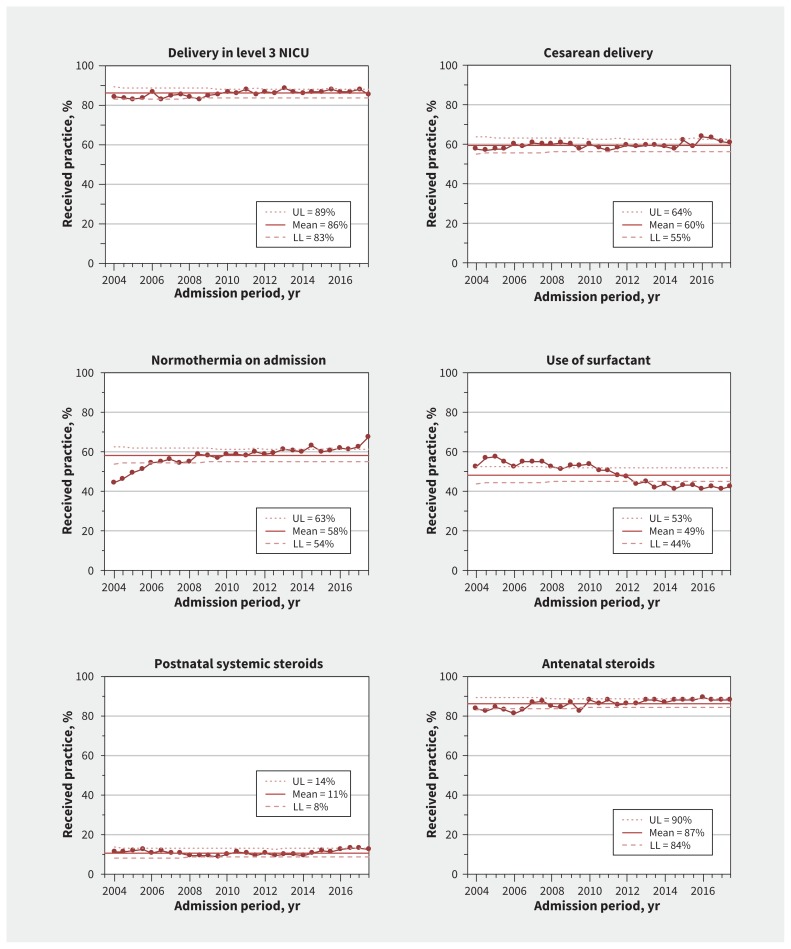
Results: The final study population included 50 831 infants. As a result of practice changes, survival without major morbidity increased significantly (56.6% [669/1183] to 70.9% [1424/2009]; adjusted odds ratio [OR] 1.08, 95% confidence interval [CI] 1.06-1.10, per year) across all gestational ages. Survival of infants born at 23-25 weeks' gestation increased (70.8% [97/137] to 74.5% [219/294]; adjusted OR 1.03, 95% CI 1.02-1.05, per year). Changes in care practices included increased use of antenatal steroids (83.6% [904/1081] to 88.1% [1747/1983]), increased rates of normothermia at admission (44.8% [520/1160] to 67.5% [1316/1951]) and reduced use of pulmonary surfactant (52.8% [625/1183] to 42.7% [857/2009]).
Interpretation: Network-wide quality-improvement activities that include better implementation of optimal care practices can yield sustained improvement in survival without morbidity in very preterm infants.
© 2020 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: None declared. The authors further declare no competing interests for the Evidence-based Practice for Improving Quality (EPIQ) Investigators group.
Figures
Comment in
-
The challenge of achieving continuous quality improvement in Canadian pediatric care.CMAJ. 2020 Jan 27;192(4):E79-E80. doi: 10.1503/cmaj.200008. CMAJ. 2020. PMID: 31995517 Free PMC article. No abstract available.
References
-
- Yeo KT, Lee QY, Quek WS, et al. Trends in morbidity and mortality of extremely preterm multiple gestation newborns. Pediatrics 2015;136:263–71. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials