

Effectiveness and cost-effectiveness of The Daily Mile on childhood weight outcomes and wellbeing: a cluster randomised controlled trial
- PMID: 31988481
- PMCID: PMC7101281
- DOI: 10.1038/s41366-019-0511-0
Effectiveness and cost-effectiveness of The Daily Mile on childhood weight outcomes and wellbeing: a cluster randomised controlled trial
Abstract
Background: The Daily Mile is designed to increase physical activity levels with children running or walking around school grounds for 15-min daily. It has been adopted by schools worldwide and endorsed as a solution to tackle obesity, despite no robust evidence of its benefits. We conducted a cluster randomised controlled trial to determine its clinical and cost-effectiveness.
Methods: Forty schools were randomly assigned (1:1) to either the Daily Mile intervention or control group in which only the usual school health and wellbeing activities were implemented. The primary outcome was BMI z-score (BMIz) at 12 months follow-up from baseline, with planned subgroup analysis to examine differential effects. Primary economic analysis outcome was incremental cost per Quality-Adjusted-Life-Year (QALY) gained.
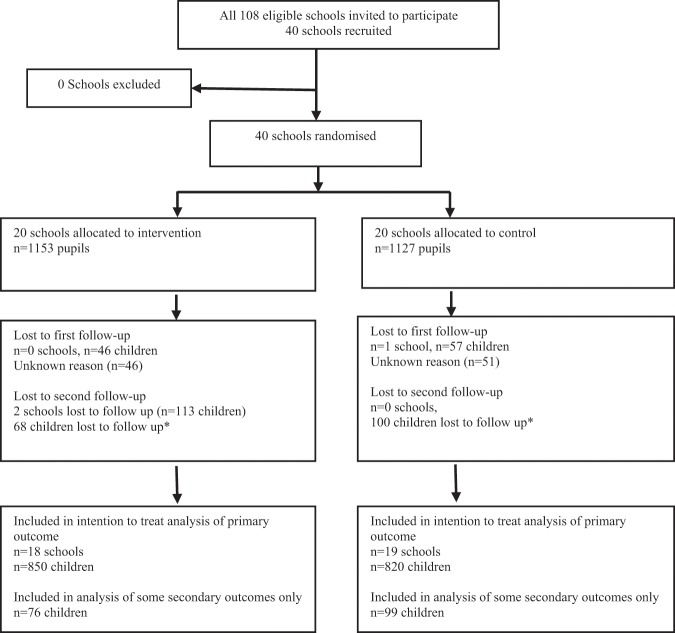
Results: Using a constrained randomisation approach, balanced on school size, baseline BMIz and proportion of pupils eligible for free school meals, 20 schools were allocated to intervention (n = 1,153 participants) and 20 to control (n = 1,127); 3 schools withdrew (2 intervention, 1 control). At 12 months, BMIz data were available for 18 intervention schools (n = 850) and 19 control schools (n = 820 participants). Using intention-to-treat analysis the adjusted mean difference (MD) in BMIz (intervention - control) was -0.036 (95% CI: -0.085 to 0.013, p = 0.146). Pre-specified subgroup analysis showed a significant interaction with sex (p = 0.001) suggesting a moderate size benefit of The Daily Mile in girls (MD -0.097, 95% CI -0.156 to -0.037). This was consistent with the exploratory economic results that showed The Daily Mile to be highly cost-effective in girls (£2,492 per QALY), but not in boys, and overall to have a 76% chance of cost-effectiveness for the whole sample, at the commonly applied UK threshold of £20,000 per QALY.
Conclusions: Overall the Daily Mile had a small but non-significant effect on BMIz, however, it had a greater effect in girls suggesting that it might be considered as a cost-effective component of a system-wide approach to childhood obesity prevention.
Conflict of interest statement
This study was funded by Birmingham City Council and was facilitated by a collaboration between Birmingham City Council, SportBirmingham, Services for Education and the University of Birmingham. The National Institute for Health Research in England under its Career Development Fellowship fund (CDF-2015-08-013) supported KB and EF. The views expressed in this publication are those of the authors and do not necessarily reflect those of the UK NHS, the National Institute for Health Research, or the Department of Health for England. EF, PA, KH, SP and EL have previously received research grants from the National Institute of Health Research; there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- World Health Organisation. Prevalence of obesity among children and adolescents. 2018. https://www.who.int/gho/ncd/risk_factors/overweight_obesity/obesity_adol....
-
- World Health Organisation. Facts and figures on childhood obesity. 2018. http://www.who.int/end-childhood-obesity/facts/en/.
-
- Dobbs R, Sawyers C, Thompson F, Manyika J, Woetzel J, Child P, et al. Overcoming obesity: an initial economic analysis. Jakarta, Indonesia: McKinsey Global Institute; 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
