

A Multidisciplinary Approach in the Management of a Paediatric Posterior Fossa Ischaemic Stroke: A Case Report
- PMID: 31988819
- PMCID: PMC6970101
- DOI: 10.7759/cureus.6418
A Multidisciplinary Approach in the Management of a Paediatric Posterior Fossa Ischaemic Stroke: A Case Report
Abstract
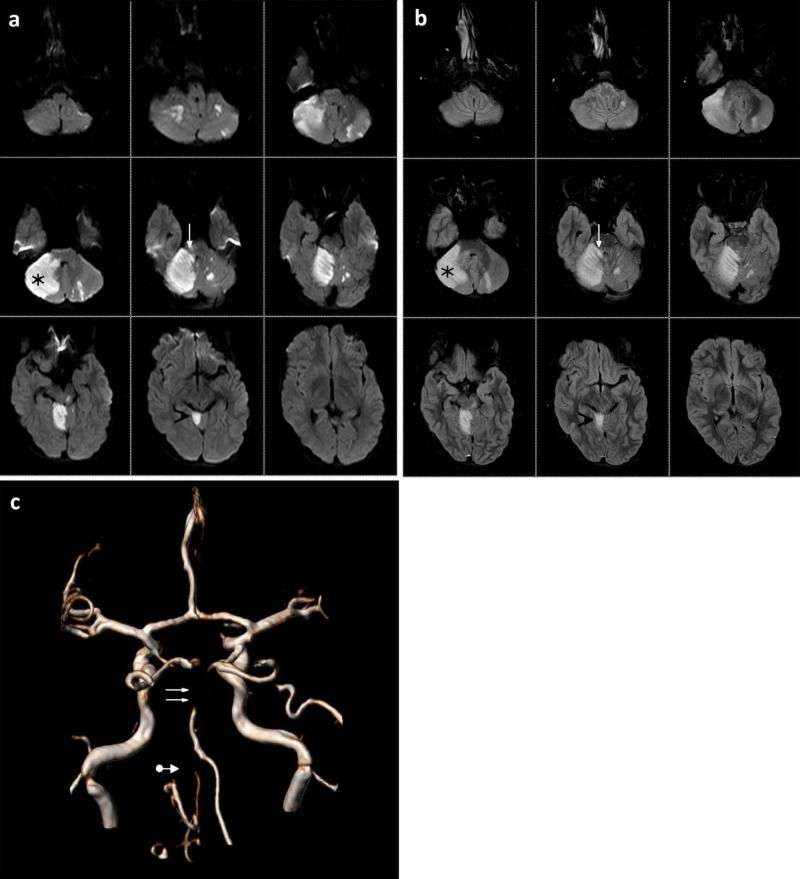
Posterior circulation acute ischaemic stroke in childhood is a rare but life-threatening disease. We describe a paediatric case of a 17-year-old Indian boy who was admitted to our centre for headache, nausea, vomiting, asthenia, and fever for two days. Computed tomography angiography (CTA), magnetic resonance angiography (MRA) and digital subtraction angiography (DSA) were performed, showing a thrombotic occlusion of the basilar artery due to focal dissection into the proximal third of the left vertebral artery. In a multidisciplinary fashion, we decided to perform a direct aspiration first pass technique (ADAPT), which led to the complete recanalization of either the left vertebral artery or the basilar artery. Twenty-four hours later, despite the anti-edemigenic medical therapy, a preventive occipital craniectomy was performed because of the presence of cerebral oedema to avoid the possible worsening of the patient and compression on the brainstem. Our experience emphasizes the importance of a multidisciplinary and preventive approach in the management of a paediatric posterior fossa ischaemic stroke.
Keywords: basilar artery occlusion; endovascular treatment; multidisciplinary approach in stroke care; occipital craniectomy; paediatric ischaemic stroke; posterior fossa ischaemic stroke; vertebral artery dissection.
Copyright © 2019, Buonomo et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



References
-
- Pediatric arterial ischemic stroke: epidemiology, risk factors, and management. Felling RJ, Sun LR, Maxwell EC, Goldenberg N, Bernard T. Blood Cells Mol Dis. 2017;67:23–33. - PubMed
-
- Endovascular mechanical thrombectomy for acute stroke in young children. Sun LR, Felling RJ, Pearl MS. J Neurointerv Surg. 2019;11:554–558. - PubMed
-
- Extracranial vertebral artery dissection in children: natural history and management. Simonnet H, Deiva K, Bellesme C, et al. Neuroradiology. 2015;57:729–738. - PubMed
-
- Childhood posterior circulation arterial ischemic stroke. Mackay MT, Prabhu SP, Coleman L. Stroke. 2010;41:2201–2209. - PubMed
Publication types
LinkOut - more resources
Full Text Sources