

Role of viruses in asthma
- PMID: 31989228
- PMCID: PMC7066101
- DOI: 10.1007/s00281-020-00781-5
Role of viruses in asthma
Abstract
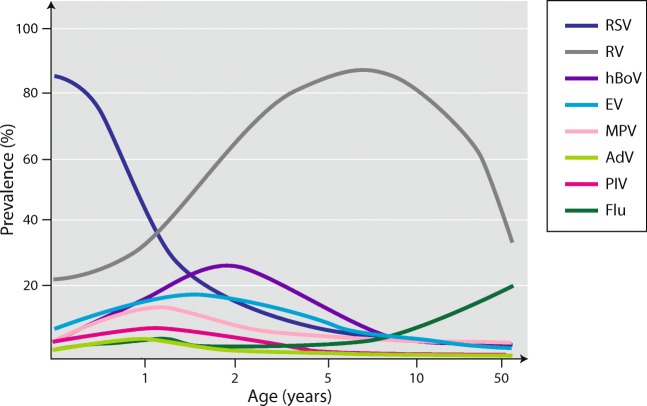
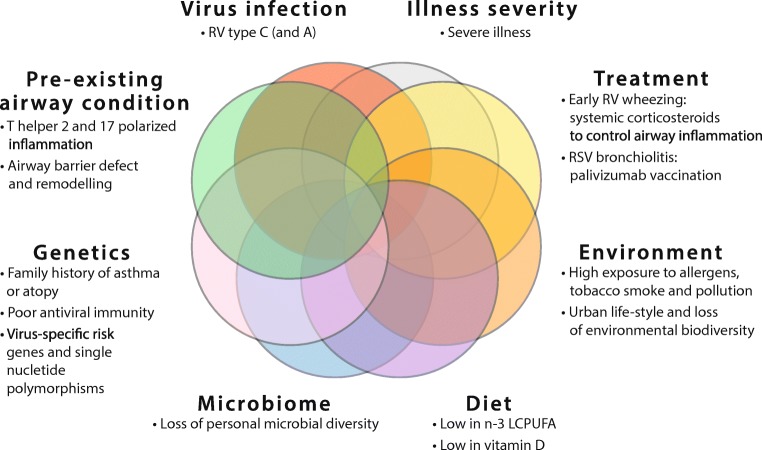
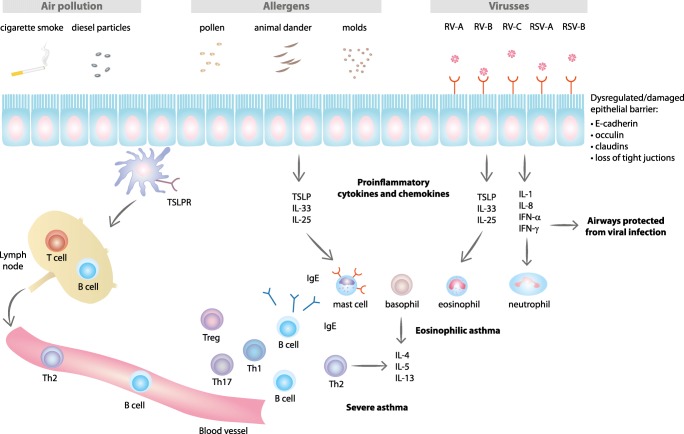
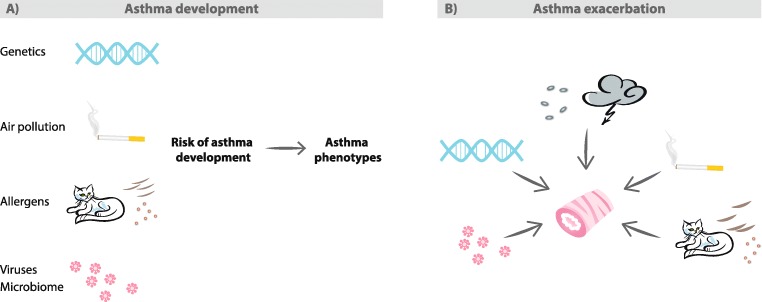
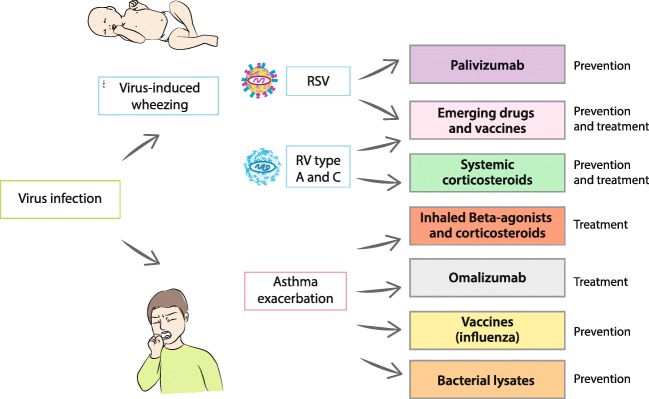
Respiratory viral infections are the most important triggers of asthma exacerbations. Rhinovirus (RV), the common cold virus, is clearly the most prevalent pathogen constantly circulating in the community. This virus also stands out from other viral factors due to its large diversity (about 170 genotypes), very effective replication, a tendency to create Th2-biased inflammatory environment and association with specific risk genes in people predisposed to asthma development (CDHR3). Decreased interferon responses, disrupted airway epithelial barrier, environmental exposures (including biased airway microbiome), and nutritional deficiencies (low in vitamin D and fish oil) increase risk to RV and other virus infections. It is intensively debated whether viral illnesses actually cause asthma. Respiratory syncytial virus (RSV) is the leading causative agent of bronchiolitis, whereas RV starts to dominate after 1 year of age. Breathing difficulty induced by either of these viruses is associated with later asthma, but the risk is higher for those who suffer from severe RV-induced wheezing. The asthma development associated with these viruses has unique mechanisms, but in general, RV is a risk factor for later atopic asthma, whereas RSV is more likely associated with later non-atopic asthma. Treatments that inhibit inflammation (corticosteroids, omalizumab) effectively decrease RV-induced wheezing and asthma exacerbations. The anti-RSV monoclonal antibody, palivizumab, decreases the risk of severe RSV illness and subsequent recurrent wheeze. A better understanding of personal and environmental risk factors and inflammatory mechanisms leading to asthma is crucial in developing new strategies for the prevention and treatment of asthma.
Keywords: Asthma; Bronchiolitis; Child; Exacerbation; Genetics; Pathogenesis; Respiratory syncytial virus; Rhinovirus; Risk; Virus; Wheeze; Wheezing.
Conflict of interest statement
WF has received speaker honoraria from Vifor Pharma. VE and KB declare that they have no conflict of interest.
Figures
References
-
- Selroos O, Kupczyk M, Kuna P, Lacwik P, Bousquet J, Brennan D, Palkonen S, Contreras J, FitzGerald M, Hedlin G, Johnston SL, Louis R, Metcalf L, Walker S, Moreno-Galdo A, Papadopoulos NG, Rosado-Pinto J, Powell P, Haahtela T. National and regional asthma programmes in Europe. Eur Respir Rev. 2015;24(137):474–483. doi: 10.1183/16000617.00008114. - DOI - PMC - PubMed
-
- Papadopoulos NG, Christodoulou I, Rohde G, Agache I, Almqvist C, Bruno A, Bonini S, Bont L, Bossios A, Bousquet J, Braido F, Brusselle G, Canonica GW, Carlsen KH, Chanez P, Fokkens WJ, Garcia-Garcia M, Gjomarkaj M, Haahtela T, Holgate ST, Johnston SL, Konstantinou G, Kowalski M, Lewandowska-Polak A, Lodrup-Carlsen K, Makela M, Malkusova I, Mullol J, Nieto A, Eller E, Ozdemir C, Panzner P, Popov T, Psarras S, Roumpedaki E, Rukhadze M, Stipic-Markovic A, Todo Bom A, Toskala E, van Cauwenberge P, van Drunen C, Watelet JB, Xatzipsalti M, Xepapadaki P, Zuberbier T (2011) Viruses and bacteria in acute asthma exacerbations--a GA2LEN-DARE systematic review. Allergy 66(4):458–468. 10.1111/j.1398-9995.2010.02505.x - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
