

Exoskeleton for post-stroke recovery of ambulation (ExStRA): study protocol for a mixed-methods study investigating the efficacy and acceptance of an exoskeleton-based physical therapy program during stroke inpatient rehabilitation
- PMID: 31992219
- PMCID: PMC6988257
- DOI: 10.1186/s12883-020-1617-7
Exoskeleton for post-stroke recovery of ambulation (ExStRA): study protocol for a mixed-methods study investigating the efficacy and acceptance of an exoskeleton-based physical therapy program during stroke inpatient rehabilitation
Abstract
Background: The ability to walk is commonly reported as a top rehabilitation priority for individuals after a stroke. However, not all individuals with stroke are able to practice walking, especially those who require more assistance from their therapist to do so. Powered robotic exoskeletons are a new generation of robotic-assisted gait training devices, designed to assist lower extremity movement to allow repetitious overground walking practice. To date, minimal research has been conducted on the use of an exoskeleton for gait rehabilitation after stroke. The following research protocol aims to evaluate the efficacy and acceptability, and thus adoptability, of an exoskeleton-based gait rehabilitation program for individuals with stroke.
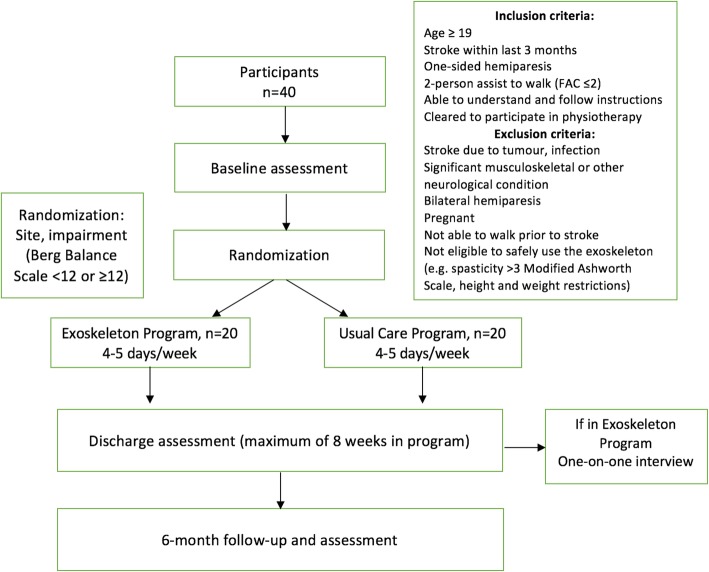
Methods: This research protocol describes a prospective, multi-center, mixed-methods study comprised of a randomized controlled trial and a nested qualitative study. Forty adults with subacute stroke will be recruited from three inpatient rehabilitation hospitals and randomized to receive either the exoskeleton-based gait rehabilitation program or usual physical therapy care. The primary outcome measure is the Functional Ambulation Category at post-intervention, and secondary outcomes include motor recovery, functional mobility, cognitive, and quality-of-life measures. Outcome data will be collected at baseline, post-intervention, and at 6 months. The qualitative component will explore the experience and acceptability of using a powered robotic exoskeleton for stroke rehabilitation from the point of view of individuals with stroke and physical therapists. Semi-structured interviews will be conducted with participants who receive the exoskeleton intervention, and with the therapists who provide the intervention. Qualitative data will be analyzed using interpretive description.
Discussion: This study will be the first mixed-methods study examining the adoptability of exoskeleton-based rehabilitation for individuals with stroke. It will provide valuable information regarding the efficacy of exoskeleton-based training for walking recovery and will shed light on how physical therapists and patients with stroke perceive the device. The findings will help guide the integration of robotic exoskeletons into clinical practice.
Trial registration: NCT02995265 (clinicaltrials.gov), Registered 16 December 2016.
Keywords: Clinical trial; Exoskeleton; Rehabilitation; Stroke; Walking.
Conflict of interest statement
The authors declare that they have no competing interests with respect to the research, the exoskeleton device manufacturer, authorship, and/or publication of this article.
Figures
References
-
- Feigin VL, Roth GA, Naghavi M, Parmar P, Krishnamurthi R, Chugh S, et al. Global burden of stroke and risk factors in 188 countries, during 1990–2013: a systematic analysis for the global burden of disease study 2013. Lancet Neurol. 2016;15:913–924. doi: 10.1016/S1474-4422(16)30073-4. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
