

Design and implementation of a clinical decision support tool for primary palliative Care for Emergency Medicine (PRIM-ER)
- PMID: 31992301
- PMCID: PMC6988238
- DOI: 10.1186/s12911-020-1021-7
Design and implementation of a clinical decision support tool for primary palliative Care for Emergency Medicine (PRIM-ER)
Abstract
Background: The emergency department is a critical juncture in the trajectory of care of patients with serious, life-limiting illness. Implementation of a clinical decision support (CDS) tool automates identification of older adults who may benefit from palliative care instead of relying upon providers to identify such patients, thus improving quality of care by assisting providers with adhering to guidelines. The Primary Palliative Care for Emergency Medicine (PRIM-ER) study aims to optimize the use of the electronic health record by creating a CDS tool to identify high risk patients most likely to benefit from primary palliative care and provide point-of-care clinical recommendations.
Methods: A clinical decision support tool entitled Emergency Department Supportive Care Clinical Decision Support (Support-ED) was developed as part of an institutionally-sponsored value based medicine initiative at the Ronald O. Perelman Department of Emergency Medicine at NYU Langone Health. A multidisciplinary approach was used to develop Support-ED including: a scoping review of ED palliative care screening tools; launch of a workgroup to identify patient screening criteria and appropriate referral services; initial design and usability testing via the standard System Usability Scale questionnaire, education of the ED workforce on the Support-ED background, purpose and use, and; creation of a dashboard for monitoring and feedback.
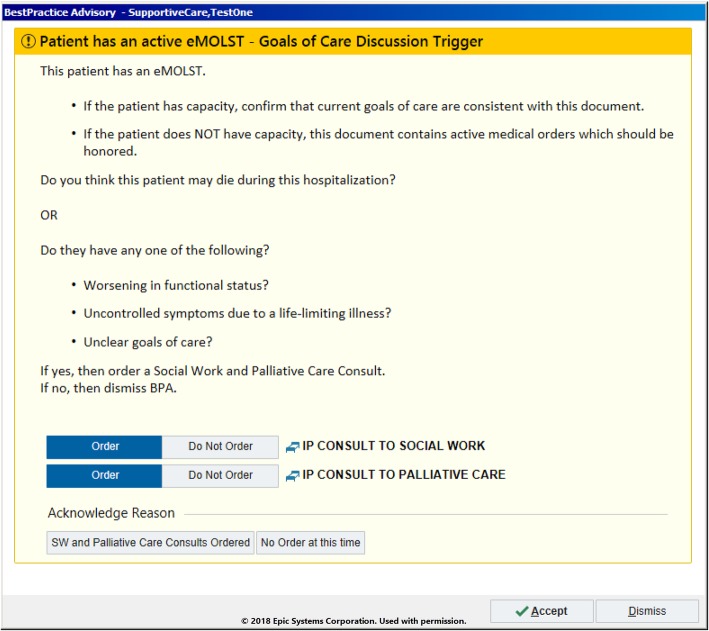
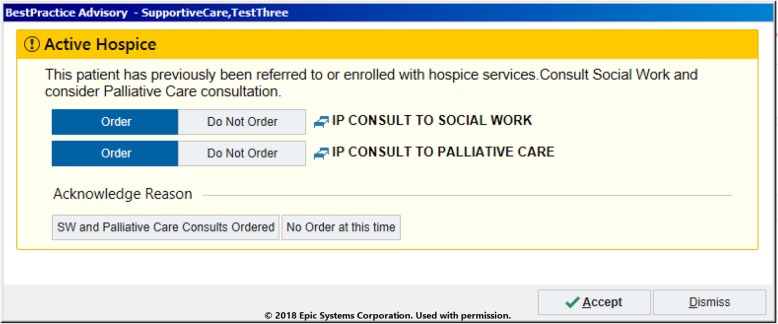
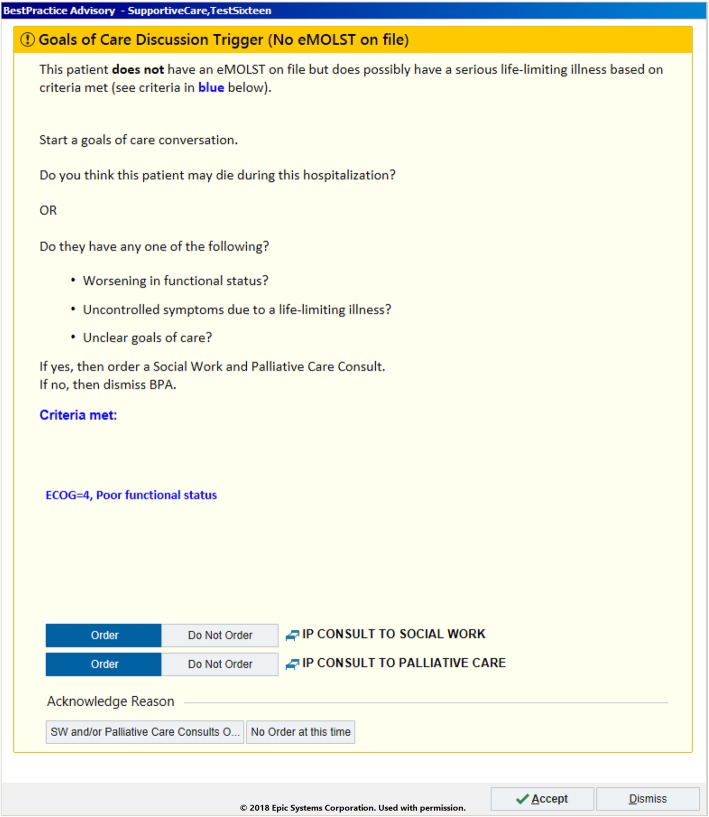
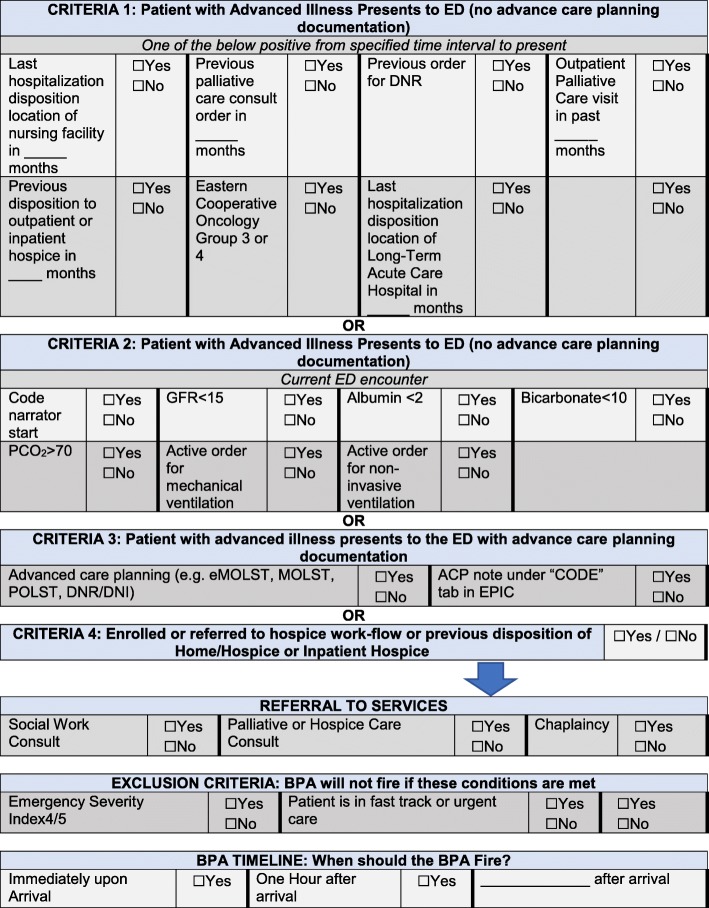
Results: The scoping review identified the Palliative Care and Rapid Emergency Screening (P-CaRES) survey as a validated instrument in which to adapt and apply for the creation of the CDS tool. The multidisciplinary workshops identified two primary objectives of the CDS: to identify patients with indicators of serious life limiting illness, and to assist with referrals to services such as palliative care or social work. Additionally, the iterative design process yielded three specific patient scenarios that trigger a clinical alert to fire, including: 1) when an advance care planning document was present, 2) when a patient had a previous disposition to hospice, and 3) when historical and/or current clinical data points identify a serious life-limiting illness without an advance care planning document present. Monitoring and feedback indicated a need for several modifications to improve CDS functionality.
Conclusions: CDS can be an effective tool in the implementation of primary palliative care quality improvement best practices. Health systems should thoughtfully consider tailoring their CDSs in order to adapt to their unique workflows and environments. The findings of this research can assist health systems in effectively integrating a primary palliative care CDS system seamlessly into their processes of care.
Trial registration: ClinicalTrials.gov Identifier: NCT03424109. Registered 6 February 2018, Grant Number: AT009844-01.
Keywords: Clinical decision support; Electronic health records; Emergency medicine; Palliative care; Quality improvement.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Coleman EA, Eilertsen TB, Kramer AM, Magid DJ, Beck A, Conner D. Reducing emergency visits in older adults with chronic illness. A randomized, controlled trial of group visits. Eff Clin Pract. 2001;4:49–57. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
