

Variability in usual care fluid resuscitation and risk-adjusted outcomes for mechanically ventilated patients in shock
- PMID: 31992351
- PMCID: PMC6986034
- DOI: 10.1186/s13054-020-2734-9
Variability in usual care fluid resuscitation and risk-adjusted outcomes for mechanically ventilated patients in shock
Abstract
Rationale: There remains significant controversy regarding the optimal approach to fluid resuscitation for patients in shock. The magnitude of care variability in shock resuscitation, the confounding effects of disease severity and comorbidity, and the relative impact on sepsis survival are poorly understood.
Objective: To evaluate usual care variability and determine the differential effect of observed and predicted fluid resuscitation volumes on risk-adjusted hospital mortality for mechanically ventilated patients in shock.
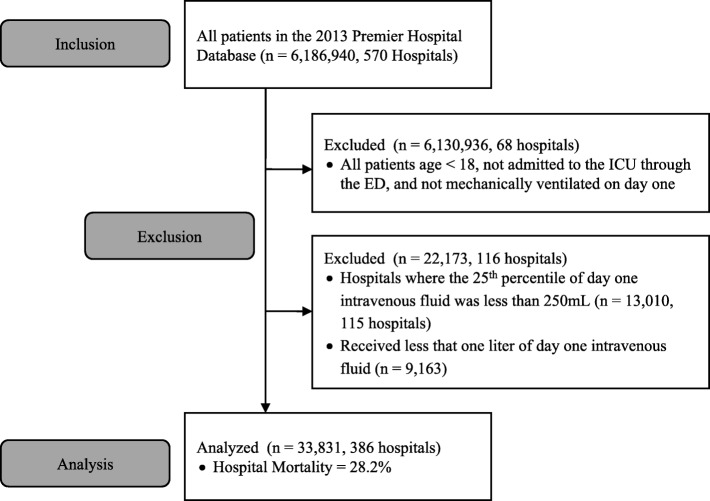
Methods: We performed a retrospective outcome analysis of mechanically ventilated patients admitted to intensive care units using the 2013 Premier Hospital Database (Premier, Inc.). Observed and predicted hospital mortality were evaluated by observed and predicted day 1 fluid administration, using the difference in predicted and observed outcomes to adjust for disease severity between groups. Both predictive models were validated using a second large administrative database (Truven Health Analytics Inc.). Secondary outcomes included duration of mechanical ventilation, hospital and ICU length of stay, and cost.
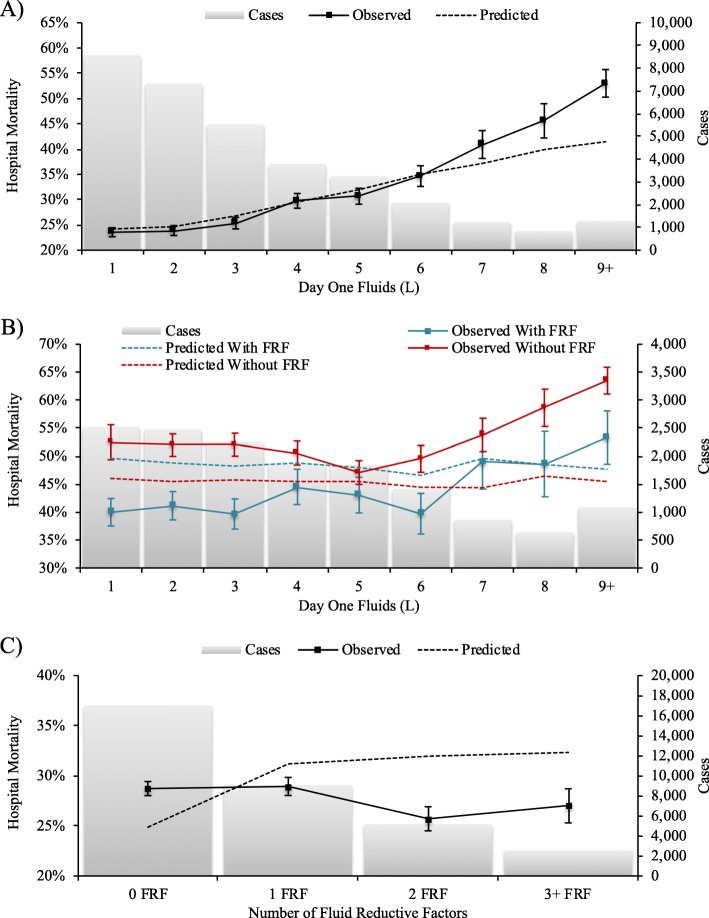
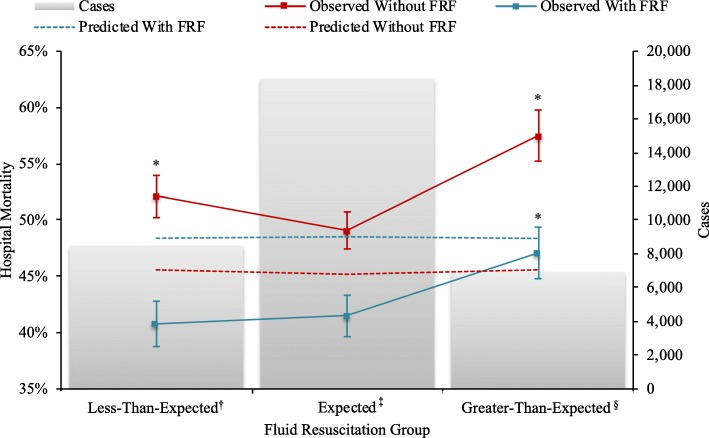
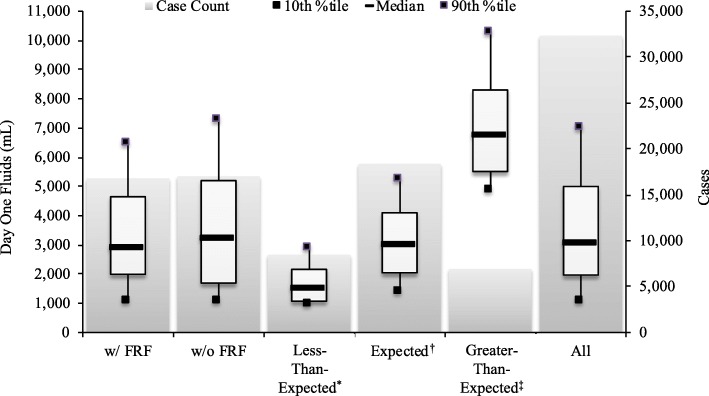
Results: Among 33,831 patients, observed hospital mortality was incrementally higher than predicted for each additional liter of day 1 fluid beginning at 7 L (40.9% vs. 37.2%, p = 0.008). Compared to patients that received expected (± 1.5 L predicted) day 1 fluid volumes, greater-than-expected fluid resuscitation was associated with increased risk-adjusted hospital mortality (52.3% vs. 45.0%, p < 0.0001) among all patients with shock and among a subgroup of shock patients with comorbid conditions predictive of lower fluid volume administration (47.1% vs. 41.5%, p < 0.0001). However, in patients with shock but without such conditions, both greater-than-expected (57.5% vs. 49.2%, p < 0.0001) and less-than-expected (52.1% vs. 49.2%, p = 0.037) day 1 fluid resuscitation were associated with increased risk-adjusted hospital mortality.
Conclusions: Highly variable day 1 fluid resuscitation was associated with a non-uniform impact on risk-adjusted hospital mortality among distinct subgroups of mechanically ventilated patients with shock. These findings support closer evaluation of fluid resuscitation strategies that include broadly applied fluid volume targets in the early phase of shock resuscitation.
Keywords: Circulatory collapse; Clinical decision-making; Critical care outcomes; Critical care/utilization; Fluid therapy/mortality.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Fluid administration in severe sepsis and septic shock, patterns and outcomes: an analysis of a large national database.Intensive Care Med. 2017 May;43(5):625-632. doi: 10.1007/s00134-016-4675-y. Epub 2017 Jan 27. Intensive Care Med. 2017. PMID: 28130687
-
Systematic assessment of fluid responsiveness during early septic shock resuscitation: secondary analysis of the ANDROMEDA-SHOCK trial.Crit Care. 2020 Jan 23;24(1):23. doi: 10.1186/s13054-020-2732-y. Crit Care. 2020. PMID: 31973735 Free PMC article.
-
Association between Initial Fluid Choice and Subsequent In-hospital Mortality during the Resuscitation of Adults with Septic Shock.Anesthesiology. 2015 Dec;123(6):1385-93. doi: 10.1097/ALN.0000000000000861. Anesthesiology. 2015. PMID: 26414499
-
Active fluid de-resuscitation in critically ill patients with septic shock: A systematic review and meta-analysis.Eur J Intern Med. 2023 Mar;109:89-96. doi: 10.1016/j.ejim.2023.01.009. Epub 2023 Jan 11. Eur J Intern Med. 2023. PMID: 36635127
-
Fluid resuscitation in circulatory shock.Crit Care Clin. 1993 Apr;9(2):313-33. Crit Care Clin. 1993. PMID: 8490765 Review.
Cited by
-
Shock Management Without Formal Fluid Responsiveness Assessment: A Retrospective Analysis of Fluid Responsiveness and Its Outcomes.J Acute Med. 2021 Dec 1;11(4):129-140. doi: 10.6705/j.jacme.202112_11(4).0002. J Acute Med. 2021. PMID: 35155089 Free PMC article.
-
Does Fluid Administration Based on Fluid Responsiveness Tests such as Passive Leg Raising Improve Outcomes in Sepsis?Curr Cardiol Rev. 2022;18(5):18-23. doi: 10.2174/1573403X18666220304202556. Curr Cardiol Rev. 2022. PMID: 35249497 Free PMC article. Review.
-
Early Restrictive or Liberal Fluid Management for Sepsis-Induced Hypotension.N Engl J Med. 2023 Feb 9;388(6):499-510. doi: 10.1056/NEJMoa2212663. Epub 2023 Jan 21. N Engl J Med. 2023. PMID: 36688507 Free PMC article. Clinical Trial.
-
The Impact of Choice Architecture on Sepsis Fluid Resuscitation Decisions: An Exploratory Survey-Based Study.MDM Policy Pract. 2022 May 14;7(1):23814683221099454. doi: 10.1177/23814683221099454. eCollection 2022 Jan-Jun. MDM Policy Pract. 2022. PMID: 35592271 Free PMC article.
-
Associations Between Volume of Early Intravenous Fluid and Hospital Outcomes in Septic Patients With and Without Heart Failure: A Retrospective Cohort Study.Crit Care Explor. 2024 Apr 26;6(5):e1082. doi: 10.1097/CCE.0000000000001082. eCollection 2024 May. Crit Care Explor. 2024. PMID: 38694845 Free PMC article.
References
-
- Malbrain ML, Marik PE, Witters I, Cordemans C, Kirkpatrick AW, Roberts DJ, et al. Fluid overload, de-resuscitation, and outcomes in critically ill or injured patients: a systematic review with suggestions for clinical practice. Anaesthesiol Intensive Ther. 2014;46(5):361–380. doi: 10.5603/AIT.2014.0060. - DOI - PubMed
-
- Kelm DJ, Perrin JT, Cartin-Ceba R, Gajic O, Schenck L, Kennedy CC. Fluid overload in patients with severe sepsis and septic shock treated with early goal-directed therapy is associated with increased acute need for fluid-related medical interventions and hospital death. Shock. 2015;43(1):68–73. doi: 10.1097/SHK.0000000000000268. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
