

Prevalence, incidence and outcomes of diabetes in Ontario First Nations children: a longitudinal population-based cohort study
- PMID: 31992559
- PMCID: PMC6996034
- DOI: 10.9778/cmajo.20190226
Prevalence, incidence and outcomes of diabetes in Ontario First Nations children: a longitudinal population-based cohort study
Abstract
Background: First Nations people are known to have a higher risk of childhood-onset type 2 diabetes, yet population-level data about diabetes in First Nations children are unavailable. In a partnership between Chiefs of Ontario and academic researchers, we describe the epidemiologic features and outcomes of diabetes in First Nations children in Ontario.
Methods: We created annual cohorts from 1995/96 to 2014/15 using data from the Registered Persons Database linked with the federal Indian Register. We used the Ontario Diabetes Database to identify children with all types of diabetes and calculated the prevalence and incidence for First Nations children and other children in Ontario. We describe glycemic control in First Nations children and other children in 2014.
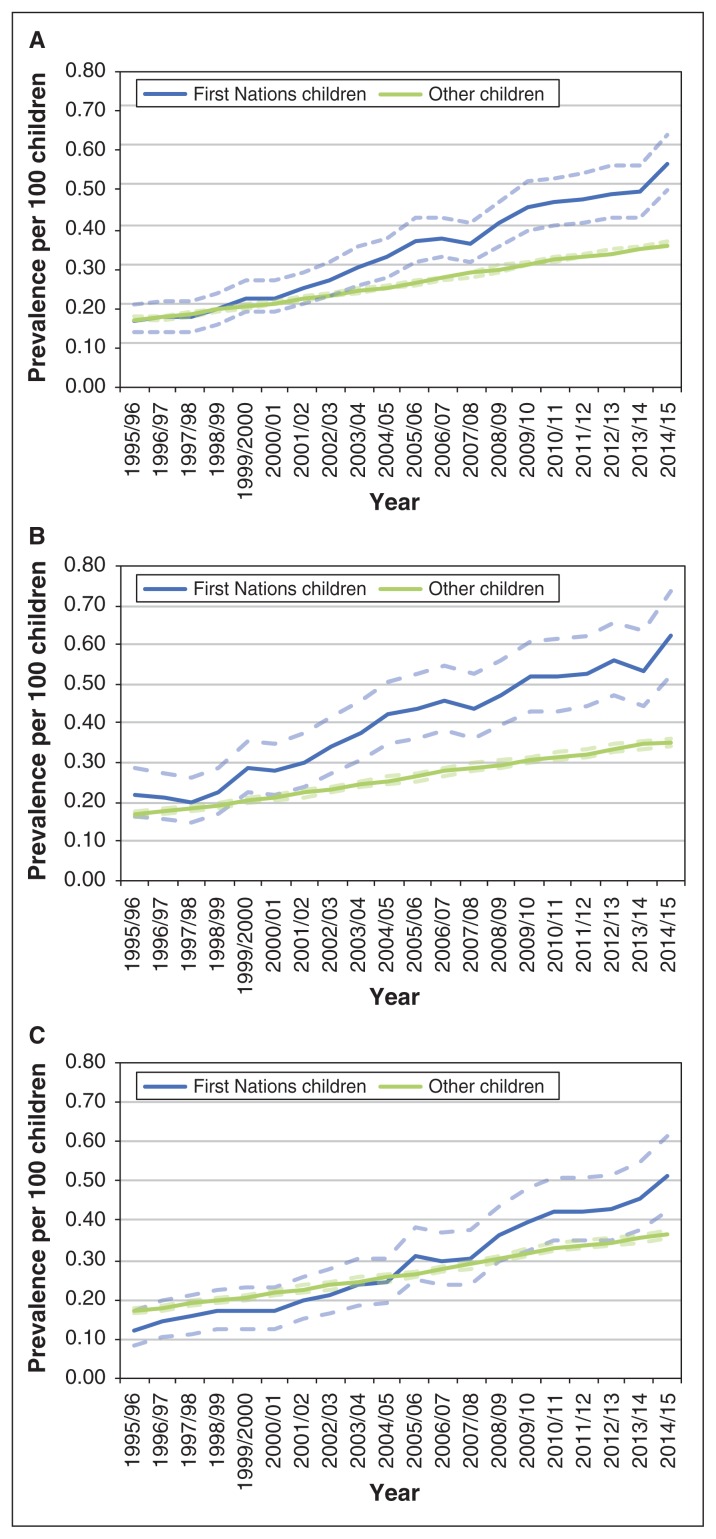
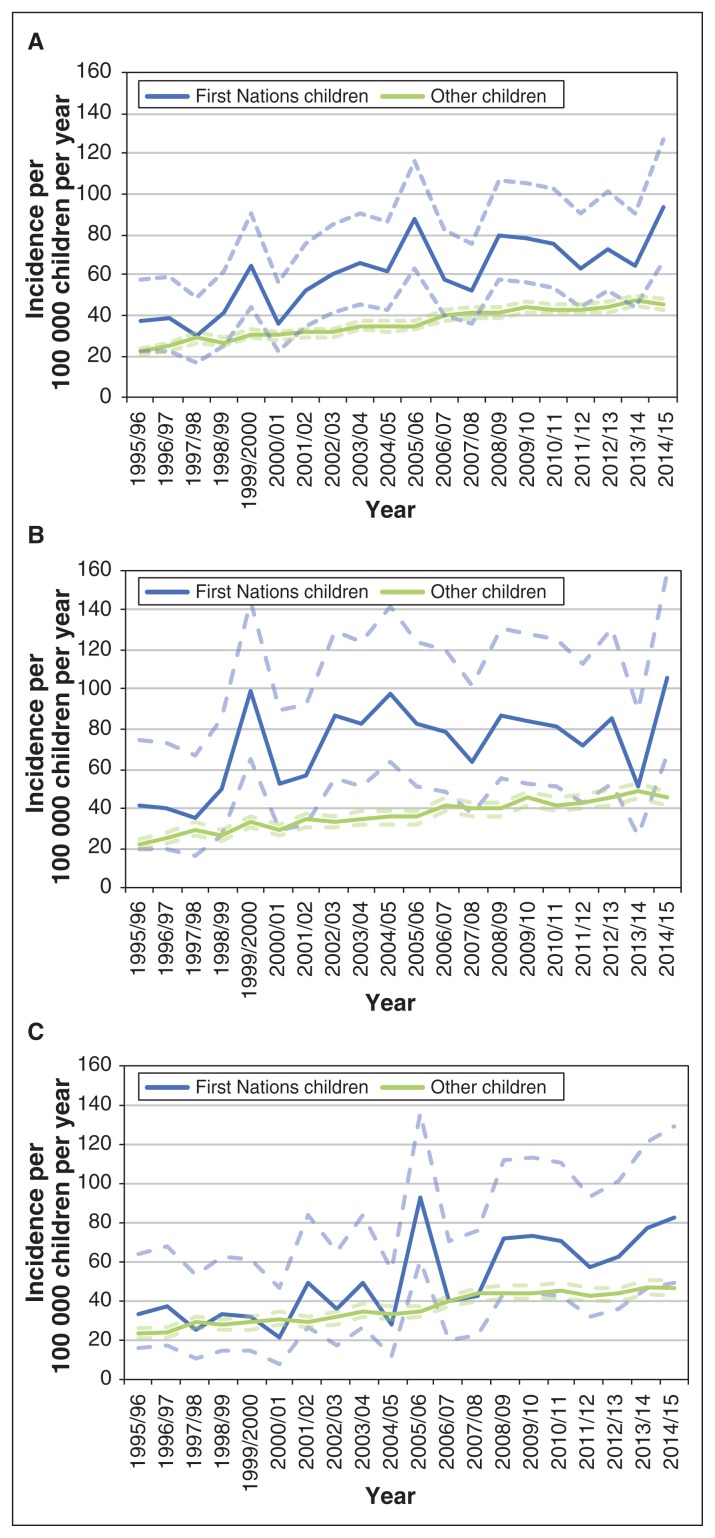
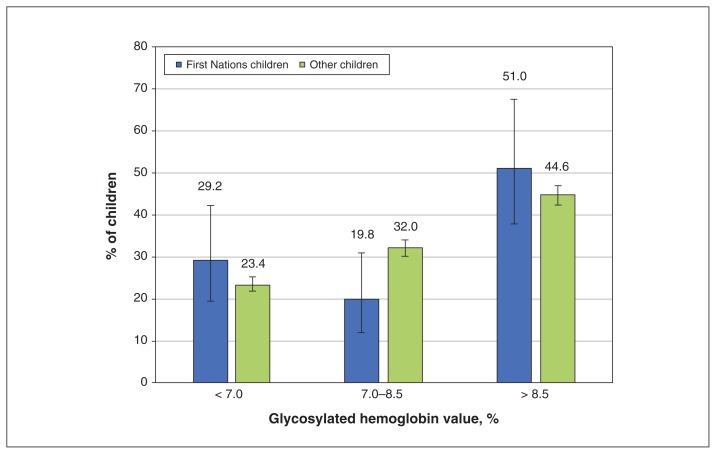
Results: In 2014/15, there were 254 First Nations children and 10 144 other children with diagnosed diabetes in Ontario. From 1995/96 to 2014/15, the prevalence increased from 0.17 to 0.57 per 100 children, and the annual incidence increased from 37 to 94 per 100 000 per year among First Nations children. In 2014/15, the prevalence of diabetes was 0.62/100 among First Nations girls and 0.36/100 among other girls. The mean glycosylated hemoglobin level among First Nations children was 9.1% (standard deviation 2.7%) and for other children, 8.5% (standard deviation 2.1%).
Interpretation: First Nations children have substantially higher rates of diabetes than non-Aboriginal children in Ontario; this is likely driven by an increased incidence of type 2 diabetes and increased risk for diabetes among First Nations girls. There is an urgent need for strategies to address modifiable factors associated with the risk of diabetes, improve access to culturally sensitive diabetes care and improve outcomes for First Nations children.
Copyright 2020, Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Michael Green reports a grant from the Ontario SPOR SUPPORT Unit during the conduct of the study and consulting fees from the First Nations and Inuit Health Branch, Health Canada outside the submitted work. No other competing interests were declared.
Figures
Comment in
- CMAJ Open. 7:E680.
References
-
- Pinhas-Hamiel O, Zeitler P. The global spread of type 2 diabetes mellitus in children and adolescents. J Pediatr. 2005;146:693–700. - PubMed
-
- Sellers EAC, Wicklow BA, Dean HJ. Clinical and demographic characteristics of type 2 diabetes in youth at diagnosis in Manitoba and northwestern Ontario (2006–2011) Can J Diabetes. 2012;36:114–8.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical