

Heart Block Caused by Cardiac Metastasis From Merkel Cell Carcinoma: A Case Report
- PMID: 31993571
- PMCID: PMC6978596
- DOI: 10.1016/j.mayocpiqo.2019.09.005
Heart Block Caused by Cardiac Metastasis From Merkel Cell Carcinoma: A Case Report
Abstract
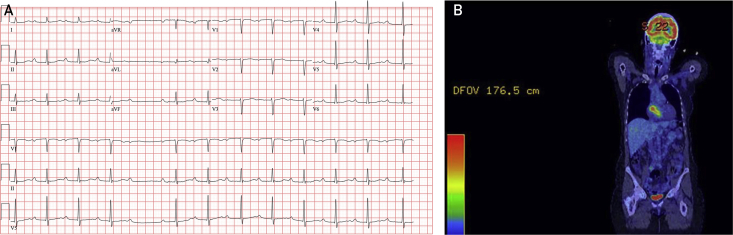
Merkel cell carcinoma (MCC) is a rare, rapidly proliferating skin cancer that commonly metastasizes to regional lymph nodes. We present the case of a 73-year-old woman with a history of MCC and non-Hodgkin B-cell lymphoma who presented with second-degree heart block (Mobitz type II) caused by an interatrial mass. Temporary pacing was required before biopsy, which revealed metastatic MCC. Treatment included permanent pacing, anti-programmed cell death ligand 1 immunotherapy, and radiation to the heart resulting in notable decrease in tumor size and normalized cardiac rhythm.
Keywords: CM, cardiac metastases; CT, computed tomography; FDG, [18F]-fluorodeoxyglucose; MCC, Merkel cell carcinoma; MCPyV, Merkel cell polyomavirus; MRI, magnetic resonance imaging; PD-L1, programmed cell death ligand 1; PET, positron emission tomography.
© 2019 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc.
Figures


References
-
- Albores-Saavedra J., Batich K., Chable-Montero F., Sagy N., Schwartz A.M., Henson D.E. Merkel cell carcinoma demographics, morphology, and survival based on 3870 cases: a population based study. J Cutan Pathol. 2010;37(1):20–27. - PubMed
-
- Wong H.H., Wang J. Merkel cell carcinoma. Arch Pathol Lab Med. 2010;134(11):1711–1716. - PubMed
-
- Warner T.F., Uno H., Hafez G.R., et al. Merkel cells and Merkel cell tumors: ultrastructure, immunocytochemistry and review of the literature. Cancer. 1983;52(2):238–245. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
