

Early antiretroviral treatment of infants to attain HIV remission
- PMID: 31993578
- PMCID: PMC6978195
- DOI: 10.1016/j.eclinm.2019.100241
Early antiretroviral treatment of infants to attain HIV remission
Abstract
Background: Studies in adults and children suggested that starting antiretroviral therapy (ART) soon after infection positively influences early events in HIV infection raising the possibility that remission may be achieved in some.
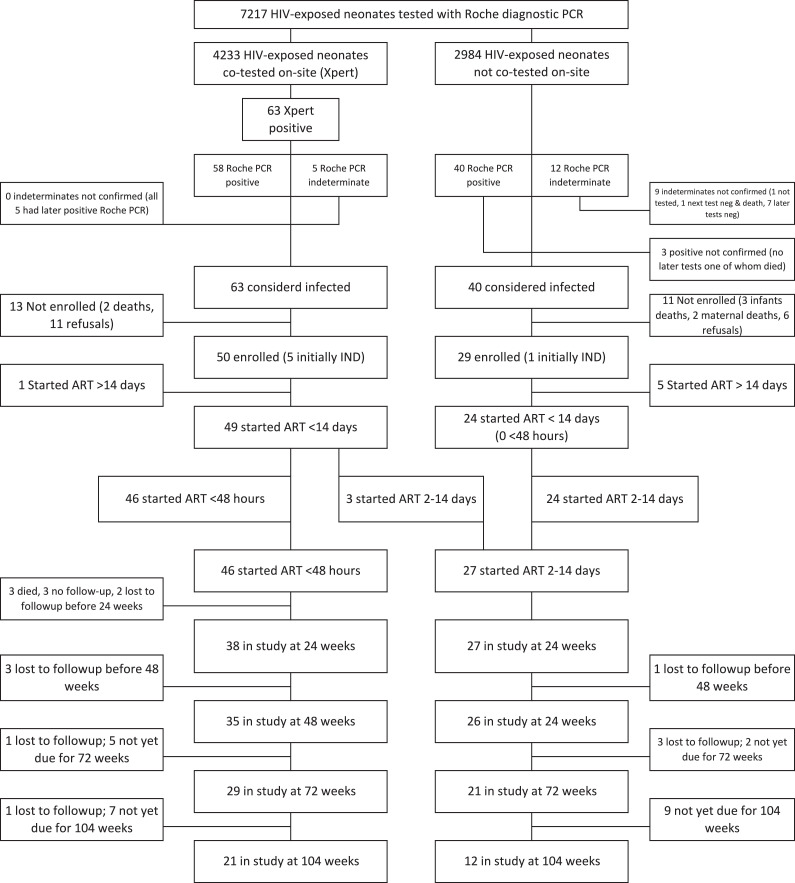
Methods: We designed an analytic treatment interruption (ATI) trial to test the hypothesis that a sizable minority of HIV-infected neonates who initiated ART <14 days of birth and maintained on ART would be able to maintain viral suppression when ART was withdrawn. To yield the target cohort for this trial, 73 HIV-infected neonates identified at one hospital in Johannesburg, South Africa, were initiated on ART <14 days of birth and maintained on ART tracking viral load (VL) decline and immune recovery (clinicaltrials.gov # NCT02431975).
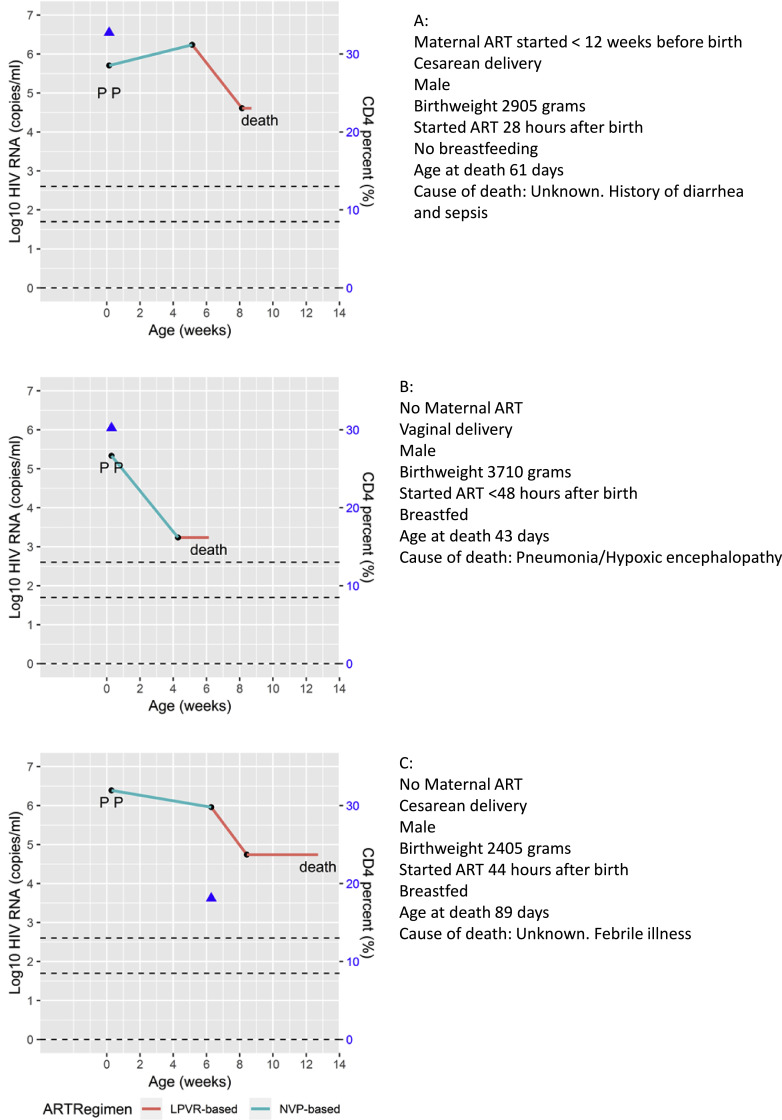
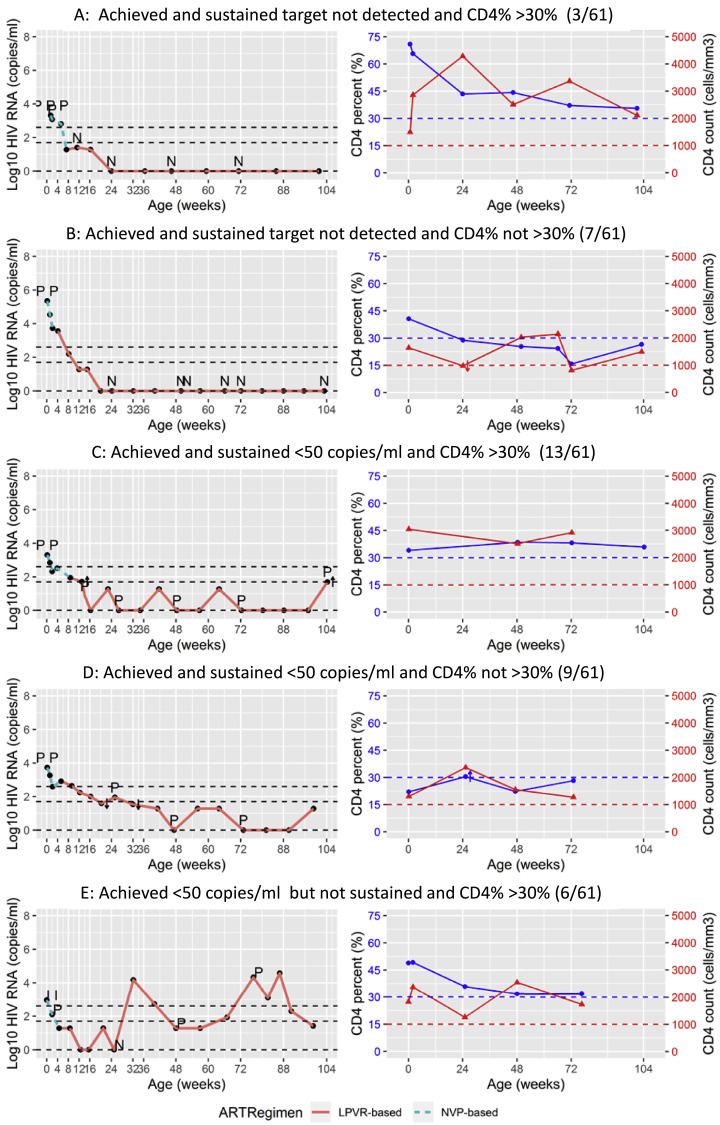
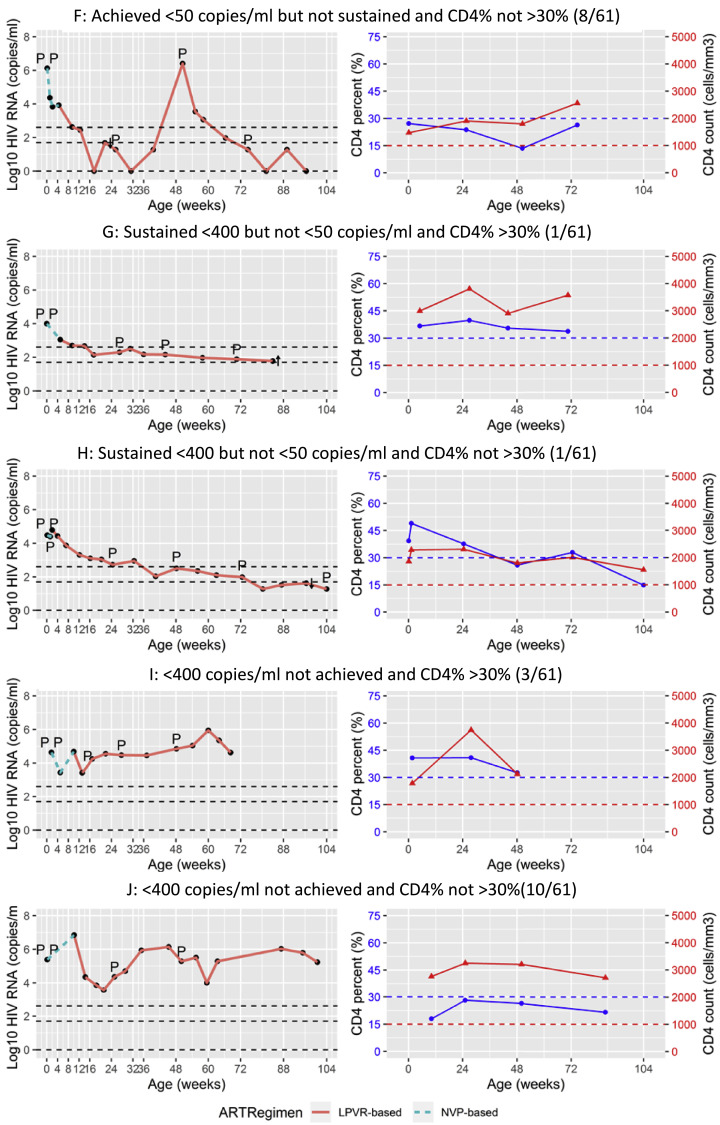
Findings: Three HIV-infected infants (4.1%) died and nine (12.3%) were lost to follow-up before 48 weeks of age. Of those surviving on study, 52.5% attained and sustained VL <50 copies/ml and half of these sustained CD4+ T-cell percentage >30% which were the primary entry criteria for the ATI trial. Proportions achieving ATI eligibility criteria were similar in the 46 infants starting ART <48 h (19.6%) to 27 infants starting 2-14 days (25.9%) (p = 0.567).
Interpretation: Very early ART on its own, using regimens available when the trial was designed, is insufficient to attain minimum entry criteria needed to justify our trial of ART interruption. Decisions about how quickly to start ART should be based on optimizing standard clinical outcomes rather than with the expectation that remission can be attained.
Funding: NICHD/NIAID (U01HD080441), South African Research Chairs Initiative of DST and NRF (South Africa).
Keywords: Antiretroviral therapy; HIV; Neonate; Remission.
© 2019 Published by Elsevier Ltd.
Conflict of interest statement
Drs. Kuhn, Technau and Coovadia report receiving grants from NIH. Dr. Abrams and Patel report receiving grants from NICHD. Dr. Burke reports receiving grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development/National Institute of Allergy and Infectious Disease, National Institutes of Health. Dr. Tiemessen reports receiving grants from the NIH and the South African Research Chairs Initiative of the Department of Science and Technology and National Research Foundation. The other authors have nothing to disclose.
Figures
References
-
- Lodi S., Meyer L., Kelleher A.D., Rosinska M., Ghosn J., Sannes M. Immunovirologic control 24 months after interruption of antiretroviral therapy initiated close to HIV seroconversion. Arch Intern Med. 2012;172(16):1252–1255. - PubMed
-
- Steingrover R., Pogany K., Fernandez Garcia E., Jurriaans S., Brinkman K., Schuitemaker H. HIV-1 viral rebound dynamics after a single treatment interruption depends on time of initiation of highly active antiretroviral therapy. AIDS. 2008;22(13):1583–1588. - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
