

The existential crisis of bipolar II disorder
- PMID: 31993793
- PMCID: PMC6987267
- DOI: 10.1186/s40345-019-0175-7
The existential crisis of bipolar II disorder
Abstract
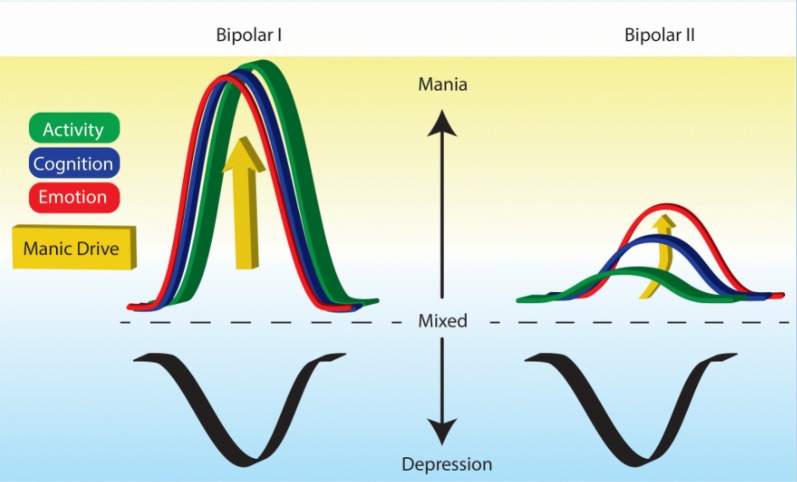
The issue of categorical vs. dimensional classification of bipolar disorder continues to generate controversy as it has for generations. Despite the evidence that no psychiatric disorder has discrete boundaries separating pathological and nonpathological states, and within a disorder, no clear differences separate subtypes-which would suggest a more dimensional approach-there are valid reasons to continue with our current categorical system, which distinguishes bipolar I from bipolar II disorder. Complicating the issue, a number of interested constituencies, including patients and their families, clinicians, scientists/researchers, and governmental agencies and insurance companies have different interests and needs in this controversy. This paper reviews both the advantages and disadvantages of continuing the bipolar I/bipolar II split vs. redefining bipolar disorder as one unified diagnosis. Even with one unified diagnosis, other aspects of psychopathology can be used to further describe and classify the disorder. These include both predominant polarity and categorizing symptoms by ACE-activity, cognition and energy. As a field, we must decide whether changing our current classification before we have a defining biology and genetic profile of bipolar disorder is worth the disruption in our current diagnostic system.
Keywords: Bipolar I; Bipolar II; Diagnosis; Nomenclature.
Conflict of interest statement
MGitlin: Not applicable.
G. Malhi: Speaker: AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier; and has been a consultant for AstraZeneca, Janssen Cilag, Lundbeck, Otsuka and Servier.
Figures
References
-
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders. 4. Washington (DC): American Psychological Association; 1994.
-
- Bond DJ, Noronha MM, Kauer-Sant’Anna M, et al. Antidepressant-associated mood elevation in bipolar Ii disorder compared with bipolar I disorder and major depressive disorder: a systematic review and meta-analysis. J Clin Psychol. 2008;69:1589–1601. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
