

Multidisciplinary patient care in X-linked hypophosphatemic rickets: one challenge, many perspectives
- PMID: 31993875
- PMCID: PMC7098922
- DOI: 10.1007/s10354-019-00732-2
Multidisciplinary patient care in X-linked hypophosphatemic rickets: one challenge, many perspectives
Abstract
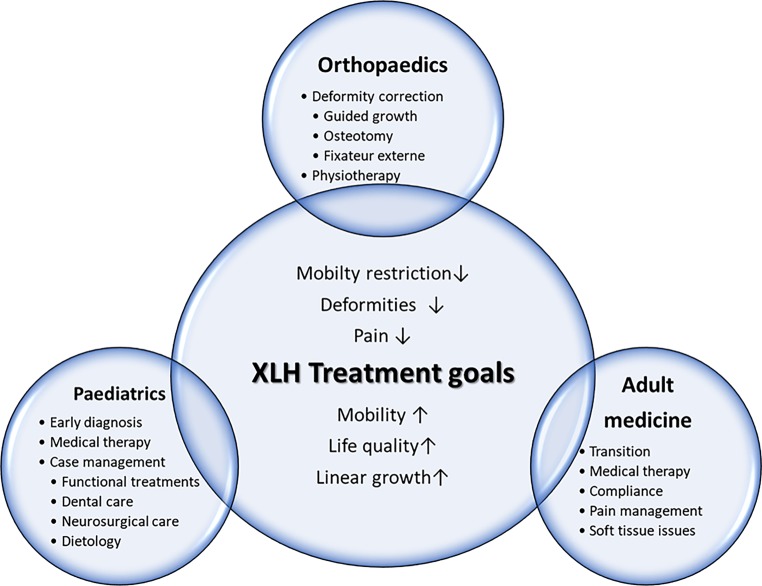
X‑linked hypophosphatemic rickets (XLH, OMIM #307800) is a rare genetic metabolic disorder caused by dysregulation of fibroblast-like growth factor 23 (FGF23) leading to profound reduction in renal phosphate reabsorption. Impaired growth, severe rickets and complex skeletal deformities are direct consequences of hypophosphatemia representing major symptoms of XLH during childhood. In adults, secondary complications including early development of osteoarthritis substantially impair quality of life and cause significant clinical burden. With the global approval of the monoclonal FGF23 antibody burosumab, a targeted treatment with promising results in phase III studies is available for children with XLH. Nevertheless, complete phenotypic rescue is rarely achieved and remaining multisystemic symptoms demand multidisciplinary specialist care. Coordination of patient management within the major medical disciplines is a mainstay to optimize treatment and reduce disease burden. This review aims to depict different perspectives in XLH patient care in the setting of a multidisciplinary centre of expertise for rare bone diseases.
Die X‑chromosomale hypophosphatämische Rachitis („X-linked hypophosphatemic rickets“, XLH: OMIM #307800) ist eine seltene genetische Erkrankung des Knochenstoffwechsels. Durch eine Dysregulation von „fibroblast-like-growth factor 23“ (FGF23) kommt es zu einem ausgeprägten renalen Phosphatverlust, der sich im Kindesalter mit reduziertem Längenwachstum, schwerer Rachitis und Deformitäten der Extremitäten manifestiert. Im Erwachsenenalter tragen das frühe Auftreten von Arthrose sowie chronische skeletale Schmerzen zur hohen Morbidität der Patienten bei. Seit der weltweiten Zulassung eines monoklonalen Antikörpers gegen FGF23, Burosumab, mit vielversprechenden Ergebnissen in Phase-III-Studien steht erstmals eine kausale Therapieoption für pädiatrische Patienten mit XLH zur Verfügung. Aufgrund der meist bestehenden Restsymptomatik ist die spezialisierte multidisziplinäre Versorgung der Patienten trotz Fortschritten in der Behandlung die essenzielle Grundlage in der langfristigen Betreuung der Patienten. Dabei spielt die Koordination der Behandlung innerhalb der wesentlichen medizinischen Fachgebiete eine wichtige Rolle für die optimale Therapie und Senkung der Krankheitslast. Diese Übersichtsarbeit gibt die verschiedenen Perspektiven der Versorgung von Patienten mit XLH aus Sicht von Mitgliedern eines nationalen Expertisezentrums für seltene Knochenerkrankungen wieder.
Keywords: Burosumab; FGF23; Phosphate; Rare disease; XLH.
Conflict of interest statement
A. Raimann, G.T. Mindler, R. Kocijan, K. Bekes, J. Zwerina, G. Haeusler and R. Ganger declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
