

Dose, Timing, and Spectrum of Prenatal Antibiotic Exposure and Risk of Childhood Asthma
- PMID: 31994697
- PMCID: PMC7850553
- DOI: 10.1093/cid/ciaa085
Dose, Timing, and Spectrum of Prenatal Antibiotic Exposure and Risk of Childhood Asthma
Erratum in
-
Correction to: Dose, Timing, and Spectrum of Prenatal Antibiotic Exposure and Risk of Childhood Asthma.Clin Infect Dis. 2022 Apr 9;74(7):1321. doi: 10.1093/cid/ciac148. Clin Infect Dis. 2022. PMID: 35297482 Free PMC article. No abstract available.
Abstract
Background: The potential for prenatal antibiotic exposure to influence asthma risk is not clear. We aimed to determine the effect of timing, dose, and spectrum of prenatal antibiotic exposure on the risk of childhood asthma.
Methods: We conducted a population-based cohort study of 84 214 mother-child dyads to examine the association of prenatal antibiotic exposure and childhood asthma using multivariable logistic regression models.
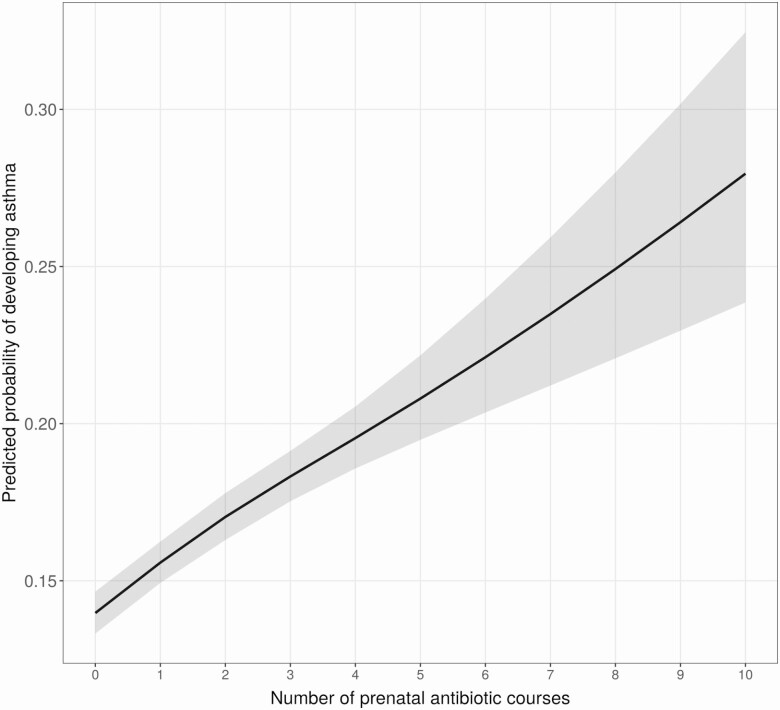
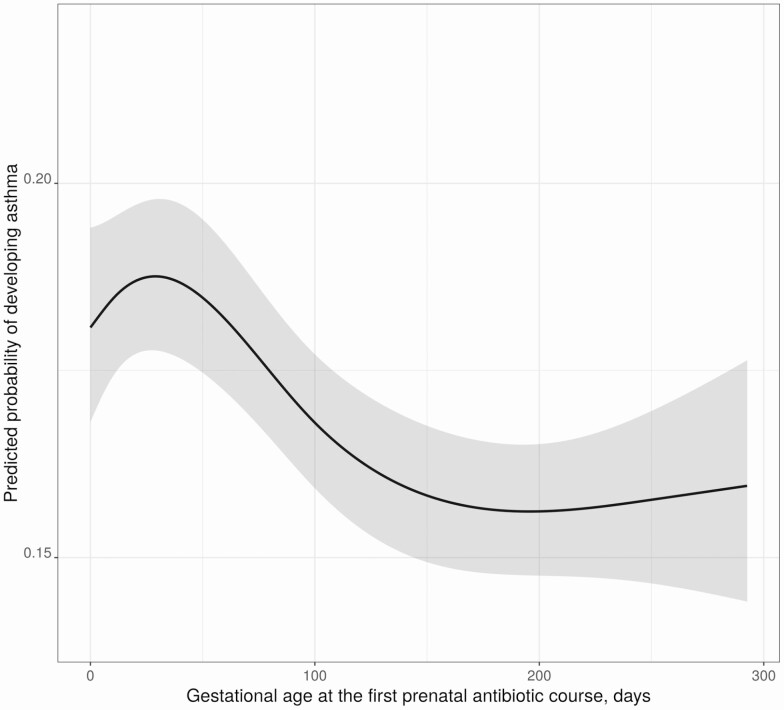
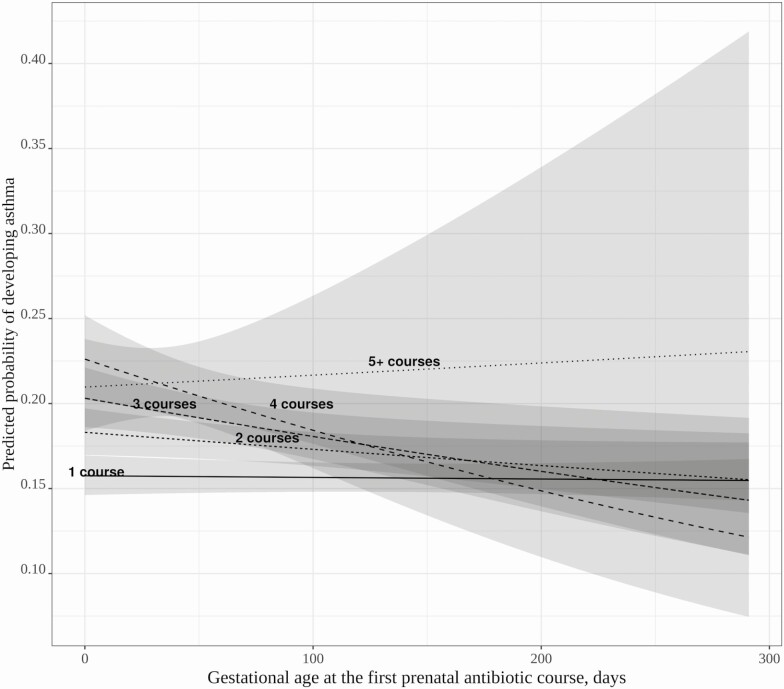
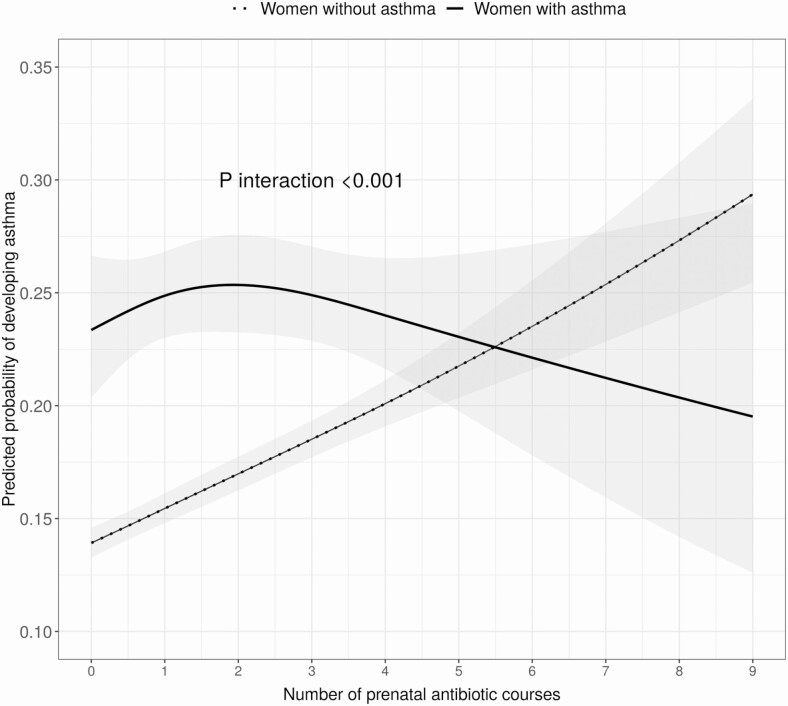
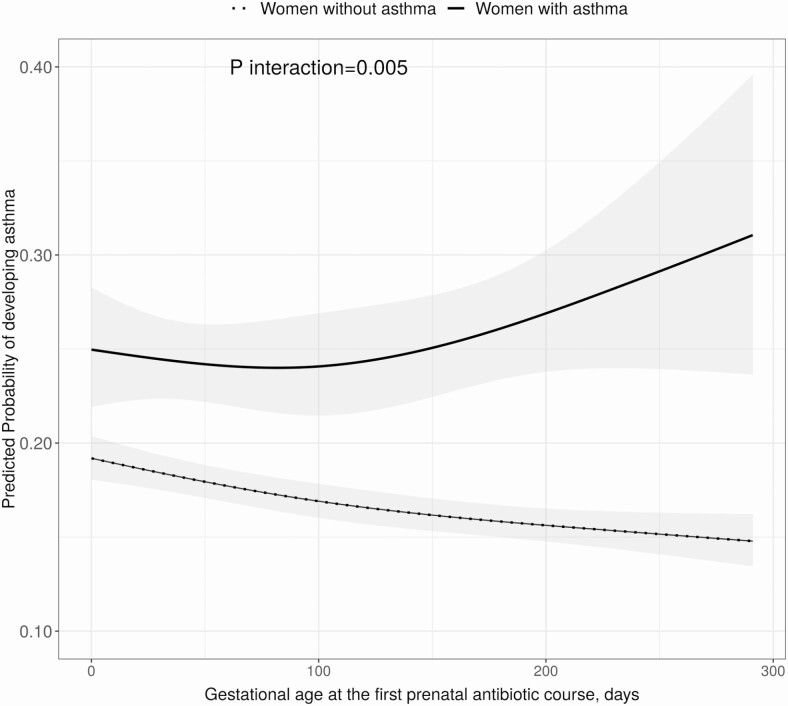
Results: Sixty-four percent of pregnant women received antibiotics. Prenatal antibiotic exposure was associated dose-dependently with increased odds of childhood asthma (adjusted odds ratio [aOR] for interquartile increase of 2 courses [interquartile range, 0-2], 1.26 [95% confidence interval {CI}, 1.20-1.33]). Among children exposed to at least 1 course in utero, the effect of timing at the first course was moderated by total maternal courses. Among pregnant women receiving a single antibiotic course, timing of exposure had no effect on childhood asthma risk. Among women receiving > 1 course, early exposure of the first course was associated with greater childhood asthma risk. Compared to narrow spectrum-only antibiotic use, broad spectrum-only antibiotic exposure was associated with increased odds of asthma (aOR, 1.14 [95% CI, 1.05-1.24]). There were effect modifications (P < .001) by maternal asthma on total courses, and on timing of the first course, significant only among those without maternal asthma.
Conclusions: Increased cumulative dose, early pregnancy first course, and broad-spectrum antibiotic exposure were associated with childhood asthma risk. Our study provides important evidence supporting judicious prenatal antibiotic use, particularly timing of use and choice of antibiotics, in preventing subsequent childhood asthma.
Keywords: prenatal antibiotic exposure; antibiotic course timing; childhood asthma; dose-response relationship; genetic predisposition.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Baïz N, Annesi-Maesano I. Is the asthma epidemic still ascending? Clin Chest Med 2012; 33:419–29. - PubMed
-
- Eder W, Ege MJ, von Mutius E. The asthma epidemic. N Engl J Med 2006; 355:2226–35. - PubMed
-
- Bookstaver PB, Bland CM, Griffin B, Stover KR, Eiland LS, McLaughlin M. A review of antibiotic use in pregnancy. Pharmacotherapy 2015; 35:1052–62. - PubMed
-
- Broe A, Pottegard A, Lamont RF, Jorgensen JS, Damkier P. Increasing use of antibiotics in pregnancy during the period 2000–2010: prevalence, timing, category, and demographics. BJOG 2014; 121:988–96. - PubMed
-
- de Jonge L, Bos HJ, van Langen IM, de Jong-van den Berg LT, Bakker MK. Antibiotics prescribed before, during and after pregnancy in the Netherlands: a drug utilization study. Pharmacoepidemiol Drug Saf 2014; 23:60–8. - PubMed
