

A systematic scoping review of clinical indications for induction of labour
- PMID: 31995603
- PMCID: PMC6988952
- DOI: 10.1371/journal.pone.0228196
A systematic scoping review of clinical indications for induction of labour
Abstract
Background: The proportion of women undergoing induction of labour (IOL) has risen in recent decades, with significant variation within countries and between hospitals. The aim of this study was to review research supporting indications for IOL and determine which indications are supported by evidence and where knowledge gaps exist.
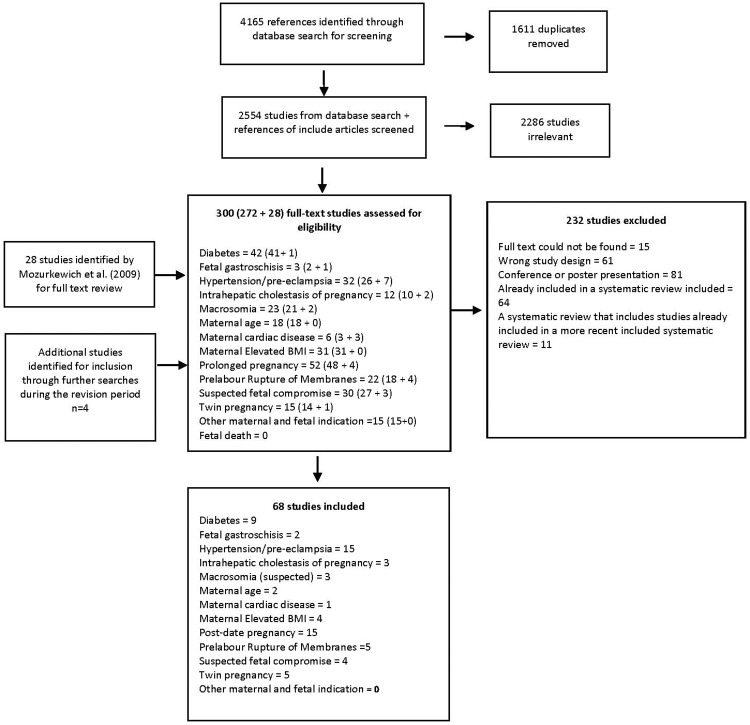
Methods: A systematic scoping review of quantitative studies of common indications for IOL. For each indication, we included systematic reviews/meta-analyses, randomised controlled trials (RCTs), cohort studies and case control studies that compared maternal and neonatal outcomes for different modes or timing of birth. Studies were identified via the databases PubMed, Maternity and Infant Care, CINAHL, EMBASE, and ClinicalTrials.gov from between April 2008 and November 2019, and also from reference lists of included studies. We identified 2554 abstracts and reviewed 300 full text articles. The quality of included studies was assessed using the RoB 2.0, the ROBINS-I and the ROBIN tool.
Results: 68 studies were included which related to post-term pregnancy (15), hypertension/pre-eclampsia (15), diabetes (9), prelabour rupture of membranes (5), twin pregnancy (5), suspected fetal compromise (4), maternal elevated body mass index (BMI) (4), intrahepatic cholestasis of pregnancy (3), suspected macrosomia (3), fetal gastroschisis (2), maternal age (2), and maternal cardiac disease (1). Available evidence supports IOL for women with post-term pregnancy, although the evidence is weak regarding the timing (41 versus 42 weeks), and for women with hypertension/preeclampsia in terms of improved maternal outcomes. For women with preterm premature rupture of membranes (24-37 weeks), high-quality evidence supports expectant management rather than IOL/early birth. Evidence is weakly supportive for IOL in women with term rupture of membranes. For all other indications, there were conflicting findings and/or insufficient power to provide definitive evidence.
Conclusions: While for some indications, IOL is clearly recommended, a number of common indications for IOL do not have strong supporting evidence. Overall, few RCTs have evaluated the various indications for IOL. For conditions where clinical equipoise regarding timing of birth may still exist, such as suspected macrosomia and elevated BMI, researchers and funding agencies should prioritise studies of sufficient power that can provide quality evidence to guide care in these situations.
Conflict of interest statement
The authors have declared that no competing interests exist.
References
-
- Centre for Epidemiology and Evidence. New South Wales Mothers and Babies 2016. Sydney: NSW Ministry of Health; 2017.
-
- McCarthy F, Kenny LC. Induction of labour. Obstetrics, Gynaecology and Reproductive Medicine. 2016;26(10):304–10.
-
- McCarthy F, Kenny L. Induction of labour. Obstetrics, Gynaecology and Reproductive Medicine. 2013;24(1):9–15.
-
- AIHW. National Maternity Data Development Project: Indications for induction of labour—Research brief no. 6. Cat. no. PER 80. Canberra: Australian Institute of Health and Welfare; 2016.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
