

Intravenous immunoglobulin for suspected or proven infection in neonates
- PMID: 31995649
- PMCID: PMC6988993
- DOI: 10.1002/14651858.CD001239.pub6
Intravenous immunoglobulin for suspected or proven infection in neonates
Abstract
Background: Neonates are at higher risk of infection due to immuno-incompetence. Maternal transport of immunoglobulins to the fetus mainly occurs after 32 weeks' gestation, and endogenous synthesis begins several months after birth. Administration of intravenous immunoglobulin (IVIG) provides immunoglobulin G (IgG) that can bind to cell surface receptors, provide opsonic activity, activate complement, promote antibody-dependent cytotoxicity and improve neutrophilic chemo-luminescence. Theoretically, infectious morbidity and mortality could be reduced by the administration of IVIG.
Objectives: To assess the effects of IVIG on mortality and morbidity caused by suspected or proven infection at study entry in neonates. To assess in a subgroup analysis the effects of IgM-enriched IVIG on mortality from suspected infection.
Search methods: For this update, MEDLINE, EMBASE, The Cochrane Library, CINAHL, trial registries, Web of Science, reference lists of identified studies, meta-analyses and personal files were searched in 2013. No language restrictions were applied.
Selection criteria: Randomised or quasi-randomised controlled trials involving newborn infants (< 28 days old); IVIG for treatment of suspected or proven bacterial or fungal infection compared with placebo or no intervention; and where one of the following outcomes was reported, mortality, length of hospital stay or psychomotor development at follow-up.
Data collection and analysis: Statistical analyses included typical risk ratio (RR), risk difference (RD), weighted mean difference (WMD), number needed to treat for an additional beneficial outcome (NNTB) or an additional harmful outcome (NNTH), all with 95% confidence intervals (CIs), and the I2 statistic to examine for statistical heterogeneity.
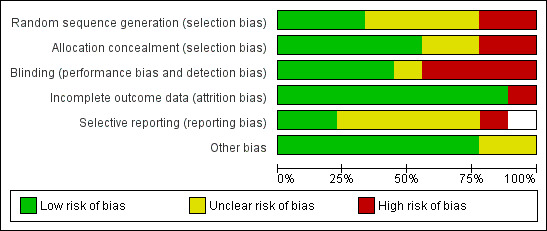
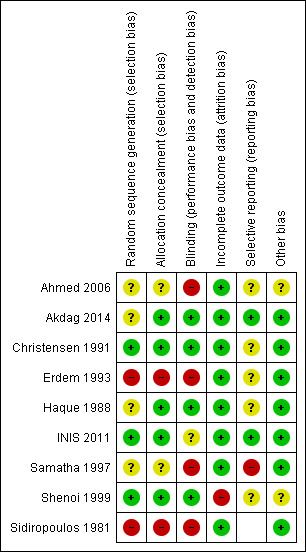
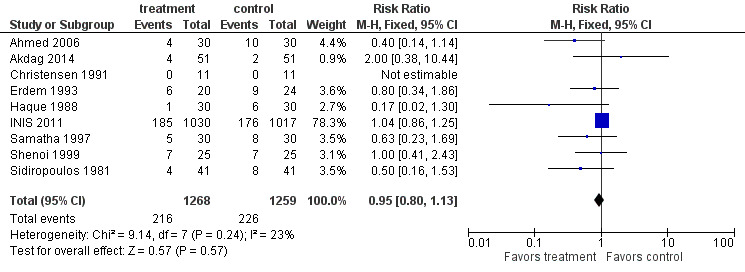
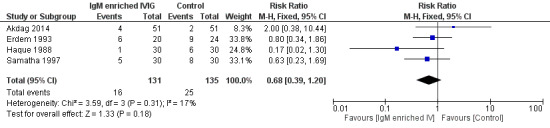
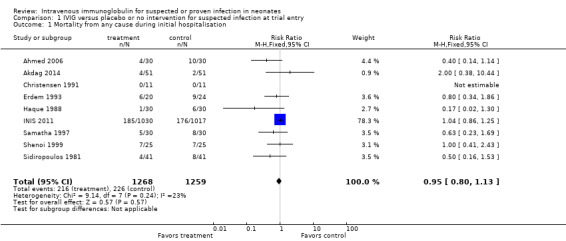
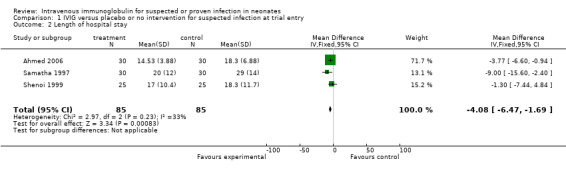
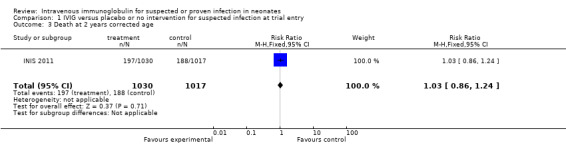
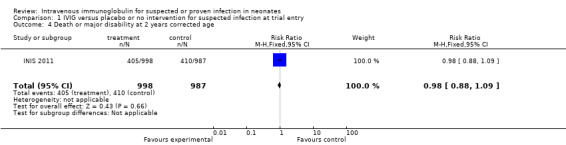
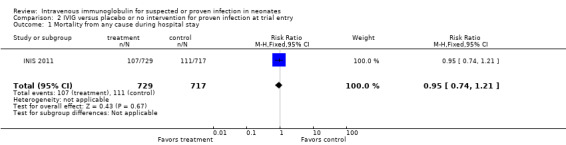
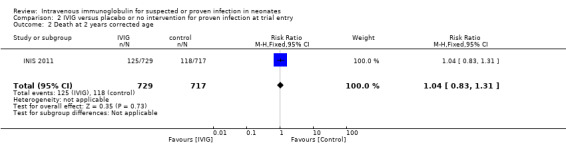
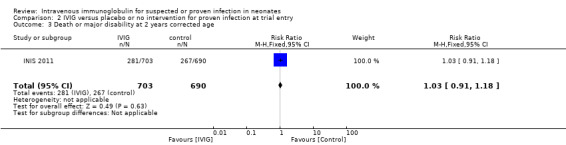
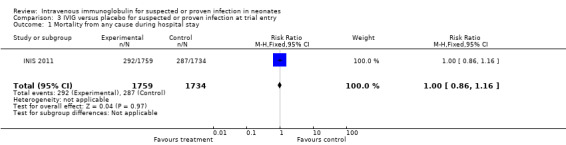
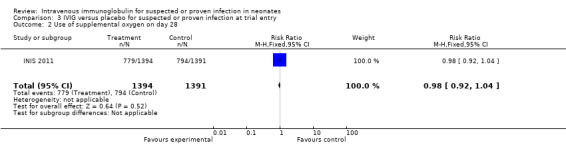
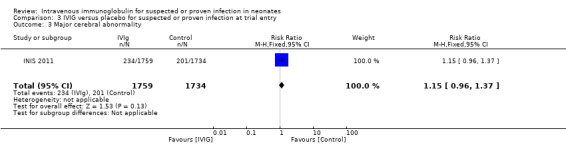
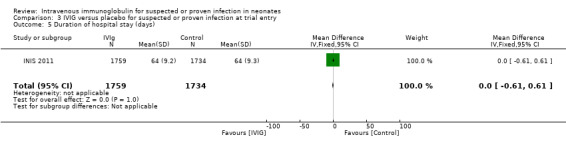
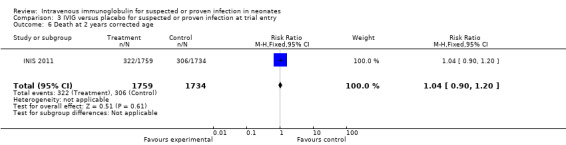
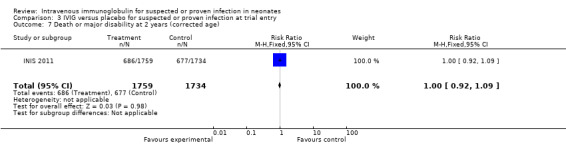
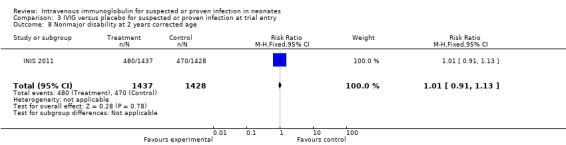
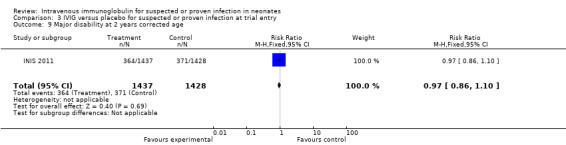
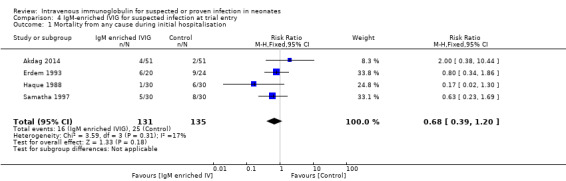
Main results: The updated search identified one published study that was previously ongoing. A total of 9 studies evaluating 3973 infants were included in this review. Mortality during hospital stay in infants with clinically suspected infection was not significantly different after IVIG treatment (9 studies (n = 2527); typical RR 0.95, 95% CI 0.80 to 1.13; typical RD -0.01, 95% CI - 0.04 to 0.02; I2 = 23% for RR and 29% for RD). Death or major disability at 2 years corrected age was not significantly different in infants with suspected infection after IVIG treatment (1 study (n = 1985); RR 0.98, 95% CI 0.88 to 1.09; RD -0.01, 95% CI -0.05 to 0.03). Mortality during hospital stay was not significantly different after IVIG treatment in infants with proven infection at trial entry (1 trial (n = 1446); RR 0.95, 95% CI 0.74 to 1.21; RD -0.01, 95% CI -0.04 to 0.03). Death or major disability at 2 years corrected age was not significantly different after IVIG treatment in infants with proven infection at trial entry (1 trial (n = 1393); RR 1.03, 95% CI 0.91 to 1.18; RD 0.01, 95% CI -0.04 to 0.06). Mortality during hospital stay in infants with clinically suspected or proven infection at trial entry was not significantly different after IVIG treatment (1 study (n = 3493); RR 1.00, 95% CI 0.86 to 1.16; RD 0.00, 95% CI - 0.02 to 0.03). Death or major disability at 2 years corrected age was not significantly different after IVIG treatment in infants with suspected or proven infection at trial entry (1 study (n = 3493); RR 1.00, 95% CI 0.92 to 1.09; RD -0.00, 95% CI -0.03 to 0.03). Length of hospital stay was not reduced for infants with suspected or proven infection at trial entry (1 study (n = 3493); mean difference (MD) 0.00 days, 95% CI -0.61 to 0.61). No significant difference in mortality during hospital stay after administration of IgM-enriched IVIG for suspected infection at trial entry was reported in 4 studies (n = 266) (typical RR 0.68, 95% CI 0.39 to 1.20; RD -0.06, 95% CI -0.14 to 0.02; I2 = 17% for RR and 53% for RD).
Authors' conclusions: The undisputable results of the INIS trial, which enrolled 3493 infants, and our meta-analyses (n = 3973) showed no reduction in mortality during hospital stay, or death or major disability at two years of age in infants with suspected or proven infection. Although based on a small sample size (n = 266), this update provides additional evidence that IgM-enriched IVIG does not significantly reduce mortality during hospital stay in infants with suspected infection. Routine administration of IVIG or IgM-enriched IVIG to prevent mortality in infants with suspected or proven neonatal infection is not recommended. No further research is recommended.
Copyright © 2020 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
None
Figures




Update of
-
Intravenous immunoglobulin for suspected or proven infection in neonates.Cochrane Database Syst Rev. 2015 Mar 27;(3):CD001239. doi: 10.1002/14651858.CD001239.pub5. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2020 Jan 29;1:CD001239. doi: 10.1002/14651858.CD001239.pub6. PMID: 25815707 Updated.
References
References to studies included in this review
Ahmed 2006 {published data only}
-
- Ahmed SS, Chowdhury MAKA, Hoque MM, Begum D, Ahmed ASMNU. Role of intravenous immunoglobulin (IVIG) as an adjuvant in the treatment of neonatal sepsis in preterm babies. Journal of Bangladesh College of Physicians and Surgeons 2006;24(3):97‐104.
Akdag 2014 {published data only}
-
- Akdag A, Dilmen U, Haque K, Dilli D, Erdeve O, Goekmen T. Role of pentoxifylline and/or IgM enriched intravenous immunoglobulin in the management of neonatal sepsis. American Journal of Perinatology 2014;31(10):905‐12. [PUBMED: 24515621] - PubMed
Christensen 1991 {published data only}
-
- Christensen RD, Brown MS, Hall DC, Lassiter HA, Hill HR. Effect of neutrophil kinetics and serum opsonic capacity of intravenous administration of immune globulin to neonates with clinical signs of early‐onset sepsis. Journal of Pediatrics 1991;118(4 Pt 1):606‐14. [PUBMED: 1901083] - PubMed
Erdem 1993 {published and unpublished data}
-
- Erdem G, Yurdakök M, Tekinalp G, Ersoy F. The use of IgM‐enriched intravenous immunoglobulin for the treatment of neonatal sepsis in preterm infants. Turkish Journal of Pediatrics 1993;35(4):277‐81. [PUBMED: 8160279] - PubMed
Haque 1988 {published and unpublished data}
-
- Haque KN, Zaidi MH, Bahakim H. IgM‐enriched intravenous immunoglobulin therapy in neonatal sepsis. American Journal of Diseases of Children 1988;142(12):1293‐6. [PUBMED: 3195529] - PubMed
INIS 2011 {published data only}
-
- INIS Collaborative Group, Brocklehurst P, Farrell B, King A, Juszczak E, Darlow B, et al. Treatment of neonatal sepsis with intravenous immune globulin. New England Journal of Medicine 2011;365(13):1201‐11. [PUBMED: 21962214] - PubMed
Samatha 1997 {published data only}
-
- Samatha S, Jalalu MP, Hegde RK, Vishwanath D, Maiya PP. Role of IgM enriched intravenous immunoglobulin as an adjuvant to antibiotics in neonatal sepsis. Karnataka Pediatric Journal 1997;11:1‐6.
Shenoi 1999 {published and unpublished data}
-
- Shenoi A, Nagesh NK, Maiya PP, Bhat SR, Rao SD. Multicenter randomized placebo controlled trial of therapy with intravenous immunoglobulin in decreasing mortality due to neonatal sepsis. Indian Pediatrics 1999;36(11):1113‐8. [PUBMED: 10745332] - PubMed
Sidiropoulos 1981 {published data only}
-
- Sidiropoulos D, Boehme U, Muralt G, Morell A, Barandun S. Immunoglobulin supplementation in prevention or treatment of neonatal sepsis. Pediatric Infectious Disease 1986;5(3 Suppl):S193‐4. [PUBMED: 3714523] - PubMed
-
- Sidiropoulos D, Bohme U, Muralt G, Morell A, Barandun S. Immunoglobulin substitution in the treatment of neonatal septicemia [Immunoglobulinsubstitution bei der Behandlung der neonatalen Sepsis]. Schweizerische Medizinische Wochenschrift 1981;111(44):1649‐55. [PUBMED: 7302548] - PubMed
References to studies excluded from this review
Chen 1996 {published data only}
-
- Chen J‐Y. Intravenous immunoglobulin in the treatment of full‐term and premature newborns with sepsis. Journal of the Formosan Medical Association 1996;95(11):839‐44. [PUBMED: 8990771] - PubMed
Gökalp 1994 {published and unpublished data}
-
- Gökalp AS, Toksoy HB, Tũrkay S, Bakici MZ, Kaya R. Intravenous immunoglobulin in the treatment of Salmonella typhimurium infections in preterm neonates. Clinical Pediatrics 1994;33(6):349‐52. [PUBMED: 8200169] - PubMed
Haque 1995 {published data only}
Mancilla‐R 1992 {published and unpublished data}
-
- Mancilla‐Ramirez J, Gonzalez‐Yunes R, Castellanos‐Cruz C, Garcia‐Roca P, Santos‐Preciado JI. Intravenous immunoglobulin in the treatment of neonatal septicemia [Immunoglobulina intravenosa en el tratamiento de septicemia neonatal]. Boletín Médico del Hospital Infantil de México 1992;49(1):4‐11. [PUBMED: 1304766] - PubMed
Salihoglu 2013 {published data only}
-
- Salihoglu Ö, Can E, Koç MÖ, Durmus E, Hatipoglu S. Pentaglobin as an adjunct therapy in very low birthweight neonates with nosocomial sepsis. Journal of the Pakistan Medical Association 2013;63(11):1353‐7. - PubMed
Weisman 1992 {published data only}
-
- Weisman LE, Stoll B, Kuesar T, Rubio T, Frank G, Heiman H. Intravenous immunoglobulin (IVIG) therapy of neonatal sepsis. Pediatric Research 1990;27:277A.
-
- Weisman LE, Stoll BJ, Kueser TJ, Rubio TT, Frank CG, Heiman HS, et al. Intravenous immune globulin therapy for early‐onset sepsis in premature neonates. Journal of Pediatrics 1992;121(3):434‐43. [PUBMED: 1517923] - PubMed
Additional references
Alejandria 2001
Alejandria 2013
Baker 1990
-
- Baker CJ. New uses of intravenous immune globulin in newborn infants. Journal of Clinical Immunology 1990;10 Suppl:47S‐55S. [PUBMED: 2081789] - PubMed
Baley 1988
-
- Baley JE. Neonatal sepsis: the potential for immunotherapy. Clinics in Perinatology 1988;15(4):755‐71. [PUBMED: 3061698] - PubMed
Baley 1992
-
- Baley JE, Fanaroff AA. Neonatal infections, Part 2: Specific infectious diseases and therapies. In: Sinclair JC, Bracken MB editor(s). Effective Care of the Newborn Infant. Oxford: Oxford University Press, 1992:477‐506.
Franco 2012
-
- Franco AC, Torrico AC, Moreira FT, Sá FP, D'Elia HV, Bernardo WM. Adjuvent use of intravenous immunoglobulin in the treatment of neonatal sepsis: a systematic review with meta‐analysis. Jornal de Pediatria (Rio J) 2012;88(5):377‐83. [PUBMED: 23002082] - PubMed
Friedman 1990
-
- Friedman CA, Wender DF, Temple DM, Rawson JE. Intravenous gamma globulin as adjunct therapy for severe group B streptococcal disease in the newborn. American Journal of Perinatology 1990;7(1):1‐4. [PUBMED: 2104748] - PubMed
Haque 1997
-
- Haque K. Should intravenous immunoglobulins be used in the treatment of neonatal sepsis?. British Journal of Intensive Care 1997;7:12‐6.
Higgins 2003
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration, 2011. www.cochrane‐handbook.org, [updated March 2011].
Hozo 2005
INIS 2008
-
- INIS Study Collaborative Group. The International Neonatal Immunotherapy Study: non‐specific intravenous immunoglobulin therapy for suspected or proven neonatal sepsis: an international, placebo controlled, multicentre randomised trial. BioMed Central Pregnancy and Childbirth 2008;8:52. [PUBMED: 19063731] - PMC - PubMed
Jenson 1997
-
- Jenson HB, Pollock BH. Meta‐analyses of the effectiveness of intravenous immune globulin for prevention and treatment of neonatal sepsis. Pediatrics 1997;99(2):e2. [PUBMED: 9099759] - PubMed
Jenson 1998
-
- Jenson HB, Pollock BH. The role of intravenous immunoglobulin for the prevention and treatment of neonatal sepsis. Seminars in Perinatology 1998;22(1):50‐63. [PUBMED: 9523399] - PubMed
Lacy 1995
Ohlsson 2013a
RevMan 2014 [Computer program]
-
- Version 5.3.3 Copenhagen: The Nordic Cochrane Center, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3.3 Copenhagen: The Nordic Cochrane Center, The Cochrane Collaboration, 2014.
Shah 2009
Stoll 1996a
-
- Stoll BJ, Gordon T, Korones SB, et al. Early‐onset sepsis in very low birth weight neonates: a report from the National Institute of Child Health and Human Development Neonatal Research Network. Journal of Pediatrics 1996;129(1):72‐80. [PUBMED: 8757565] - PubMed
Stoll 1996b
-
- Stoll BJ, Gordon T, Korones SB, et al. Late‐onset sepsis in very low birth weight neonates: a report from the National Institute of Child Health and Human Development Neonatal Research Network. Journal of Pediatrics 1996;129(1):63‐71. [PUBMED: 8757564] - PubMed
References to other published versions of this review
Ohlsson 1998b
Ohlsson 2001
Ohlsson 2004
Ohlsson 2010
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous