

An integrated intervention for chronic care management in rural Nepal: protocol of a type 2 hybrid effectiveness-implementation study
- PMID: 31996250
- PMCID: PMC6990567
- DOI: 10.1186/s13063-020-4063-3
An integrated intervention for chronic care management in rural Nepal: protocol of a type 2 hybrid effectiveness-implementation study
Abstract
Background: In Nepal, the burden of noncommunicable, chronic diseases is rapidly rising, and disproportionately affecting low and middle-income countries. Integrated interventions are essential in strengthening primary care systems and addressing the burden of multiple comorbidities. A growing body of literature supports the involvement of frontline providers, namely mid-level practitioners and community health workers, in chronic care management. Important operational questions remain, however, around the digital, training, and supervisory structures to support the implementation of effective, affordable, and equitable chronic care management programs.
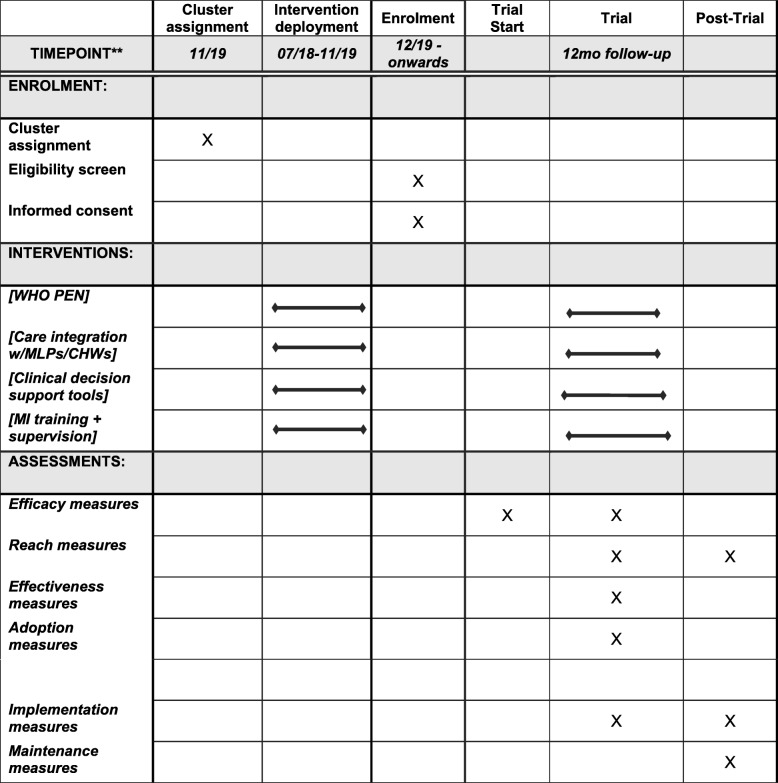
Methods: A 12-month, population-level, type 2 hybrid effectiveness-implementation study will be conducted in rural Nepal to evaluate an integrated noncommunicable disease care management intervention within Nepal's new municipal governance structure. The intervention will leverage the government's planned roll-out of the World Health Organization's Package of Essential Noncommunicable Disease Interventions (WHO-PEN) program in four municipalities in Nepal, with a study population of 80,000. The intervention will leverage both the WHO-PEN and its cardiovascular disease-specific technical guidelines (HEARTS), and will include three evidence-based components: noncommunicable disease care provision using mid-level practitioners and community health workers; digital clinical decision support tools to ensure delivery of evidence-based care; and training and digitally supported supervision of mid-level practitioners to provide motivational interviewing for modifiable risk factor optimization, with a focus on medication adherence, and tobacco and alcohol use. The study will evaluate effectiveness using a pre-post design with stepped implementation. The primary outcomes will be disease-specific, "at-goal" metrics of chronic care management; secondary outcomes will include alcohol and tobacco consumption levels.
Discussion: This is the first population-level, hybrid effectiveness-implementation study of an integrated chronic care management intervention in Nepal. As low and middle-income countries plan for the Sustainable Development Goals and universal health coverage, the results of this pragmatic study will offer insights into policy and programmatic design for noncommunicable disease care management in the future.
Trial registration: ClinicalTrials.gov, NCT04087369. Registered on 12 September 2019.
Keywords: Chronic illness; Community health workers; Decision support systems; Motivational interviewing; Nepal; Noncommunicable diseases; Rural health.
Conflict of interest statement
This study has been approved by the Ethical Review Board of the Nepal Health Research Council (#177/2018). Within the study, all patients will provide verbal informed consent to have their de-identified data analyzed and published. Care provision will be unrelated to consent, and there will be no difference in care provision based on consent status. Verbal informed consent will also be provided by all KII and FGD participants. No incentives will be provided to study participants, to avoid any conflict of interest or coercion to participate.
PA, AA, DC, BD, BG, TG, UK, PR, SS, and AT are employed by, and DS, BA, NC, SH, SM, RS, and DM work in partnership with, a nonprofit healthcare company (Nyaya Health Nepal, with support from the US-based nonprofit organization, Possible) that delivers free healthcare in rural Nepal using funds from the Government of Nepal and other public, philanthropic, and private foundation sources. DS and RS are employed at an academic medical center (Brigham and Women’s Hospital) that receives public-sector research funding, as well as revenue through private-sector fee-for-service medical transactions and private foundation grants. DS and RS are faculty members at a private medical school (Harvard Medical School). DS is employed at an academic medical center (Beth Israel Deaconess Medical Center) that receives public-sector research funding, as well as revenue through private-sector fee-for-service medical transactions and private foundation grants. DS is employed at an academic research center (Ariadne Labs) that is jointly supported by an academic medical center (Brigham and Women’s Hospital) and a private university (Harvard T.H. Chan School of Public Health) via public-sector research funding and private philanthropy. SD is a medical resident at a private academic medical center (Hurley Medical Center) that receives revenue through private-sector fee-for-service medical transactions and a charitable private foundation. AK is a medical resident at a private academic medical center (NYU Langone Health) that receives public-sector research funding, as well as revenue through private-sector fee-for-service medical transactions and private foundation grants. BA is a faculty member at a public university (University of California, San Francisco). AA is a fellow supported by a public-sector research fellowship affiliated at, and BKa and AS are faculty members at, a private university (Kathmandu University). DC is a faculty member at, SH is a graduate student at, and DC and SH are employed part-time at a public university (University of Washington). AB, DC, SK, SM, SS, and DM are faculty members at, and NC, SH, and EL are employed by, a private medical school (Icahn School of Medicine at Mount Sinai). MD is employed by the Government of Nepal (Ministry of Health and Population, Nepal Health Research Council). TG is a fellow with a bidirectional fellowship program (HEAL Initiative) that is affiliated with a public university (University of California, San Francisco) that receives funding from public, philanthropic, and private foundation sources. BKa is a faculty member at a public research university (Sun Yat-sen University). SK is the founding Executive Director at an advocacy and leadership network (Young Professionals Chronic Disease Network) that receives funding from individual philanthropy. SK serves as a consultant for Resolve To Save Lives on hypertension treatment and leads a partnership on multiple chronic conditions through his institution and Teva Pharmaceuticals. BKo is a faculty member at a public university (Tribhuvan University, Institute of Medicine). SM is a voting member on the Board of Directors with Group Care Global, a position for which she receives no compensation. RS is employed at an academic medical center (Massachusetts General Hospital) that receives public-sector research funding, as well as revenue through private-sector fee-for-service medical transactions and private foundation grants. AS is a faculty member at a private university (Yale School of Public Health). DM is a nonvoting member on Possible’s Board of Directors, a position for which he receives no compensation. All authors have read and understood
Figures
Similar articles
-
An integrated community health worker intervention in rural Nepal: a type 2 hybrid effectiveness-implementation study protocol.Implement Sci. 2018 Mar 29;13(1):53. doi: 10.1186/s13012-018-0741-x. Implement Sci. 2018. PMID: 29598824 Free PMC article.
-
The power of peers: an effectiveness evaluation of a cluster-controlled trial of group antenatal care in rural Nepal.Reprod Health. 2019 Oct 22;16(1):150. doi: 10.1186/s12978-019-0820-8. Reprod Health. 2019. PMID: 31640770 Free PMC article.
-
An effectiveness-implementation hybrid trial study protocol targeting posttraumatic stress disorder and comorbidity.Implement Sci. 2016 Apr 30;11:58. doi: 10.1186/s13012-016-0424-4. Implement Sci. 2016. PMID: 27130272 Free PMC article. Clinical Trial.
-
Transforming Nepal's primary health care delivery system in global health era: addressing historical and current implementation challenges.Global Health. 2022 Jan 31;18(1):8. doi: 10.1186/s12992-022-00798-5. Global Health. 2022. PMID: 35101073 Free PMC article. Review.
-
The Minderoo-Monaco Commission on Plastics and Human Health.Ann Glob Health. 2023 Mar 21;89(1):23. doi: 10.5334/aogh.4056. eCollection 2023. Ann Glob Health. 2023. PMID: 36969097 Free PMC article. Review.
Cited by
-
Building linkages between private pharmacies and public facilities to improve diabetes and hypertension care in urban areas of Nepal: a protocol for implementation research.Arch Public Health. 2025 Jun 19;83(1):160. doi: 10.1186/s13690-025-01586-4. Arch Public Health. 2025. PMID: 40537852 Free PMC article.
-
Health sector readiness for the prevention and control of non-communicable diseases: A multi-method qualitative assessment in Nepal.PLoS One. 2022 Sep 30;17(9):e0272361. doi: 10.1371/journal.pone.0272361. eCollection 2022. PLoS One. 2022. PMID: 36178897 Free PMC article. Review.
-
Doctor Clerk Implementation in Rural Community Hospitals for Effective Task Shifting of Doctors: A Grounded Theory Approach.Int J Environ Res Public Health. 2022 Aug 12;19(16):9944. doi: 10.3390/ijerph19169944. Int J Environ Res Public Health. 2022. PMID: 36011579 Free PMC article.
-
Theory-based mobile phone text messaging intervention for blood pressure control (TEXT4BP) among hypertensive patients in Nepal: study protocol for a feasibility randomised controlled trial.BMJ Open. 2020 Sep 1;10(9):e040799. doi: 10.1136/bmjopen-2020-040799. BMJ Open. 2020. PMID: 32873686 Free PMC article.
-
Does the place of residence influence your risk of being hypertensive? A study-based on Nepal Demographic and Health Survey.Hypertens Res. 2023 Jun;46(6):1363-1374. doi: 10.1038/s41440-023-01217-x. Epub 2023 Mar 8. Hypertens Res. 2023. PMID: 36890270 Free PMC article.
References
-
- Kyu HH, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1859–1922. doi: 10.1016/S0140-6736(18)32335-3. - DOI - PMC - PubMed
-
- Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788. doi: 10.1016/S0140-6736(18)32203-7. - DOI - PMC - PubMed
-
- Global status report on noncommunicable diseases 2014. Geneva: World Health Organization; 2014.
-
- Bloom DE, Cafiero ET, Jané-Llopis E, Abrahams-Gessel S, Bloom LR, Fathima S, et al. The global economic burden of noncommunicable diseases. Geneva: World Economic Forum and Harvard School of Public Health; 2011.
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
