

Opioid prescribing patterns among medical providers in the United States, 2003-17: retrospective, observational study
- PMID: 31996352
- PMCID: PMC7190021
- DOI: 10.1136/bmj.l6968
Opioid prescribing patterns among medical providers in the United States, 2003-17: retrospective, observational study
Abstract
Objective: To examine the distribution and patterns of opioid prescribing in the United States.
Design: Retrospective, observational study.
Setting: National private insurer covering all 50 US states and Washington DC.
Participants: An annual average of 669 495 providers prescribing 8.9 million opioid prescriptions to 3.9 million patients from 2003 through 2017.
Main outcome measures: Standardized doses of opioids in morphine milligram equivalents (MMEs) and number of opioid prescriptions.
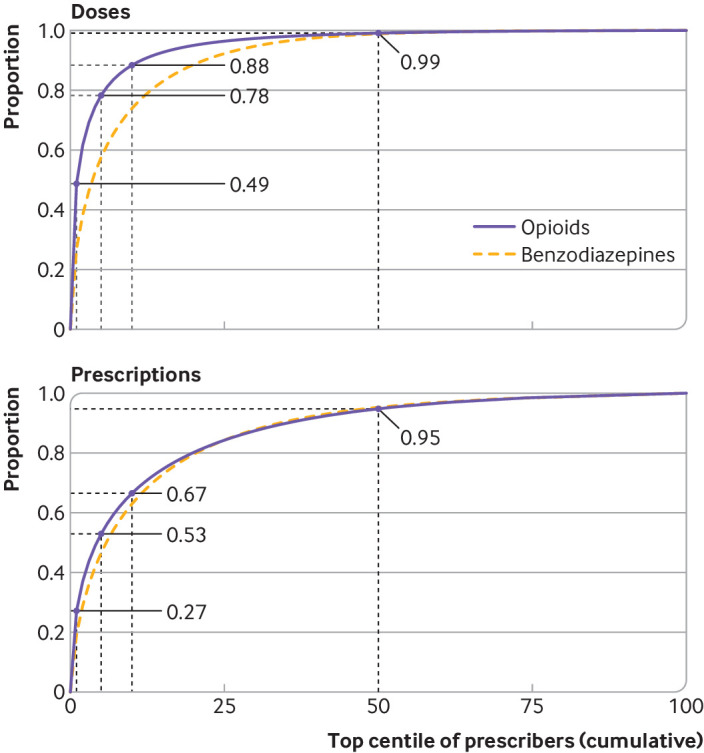
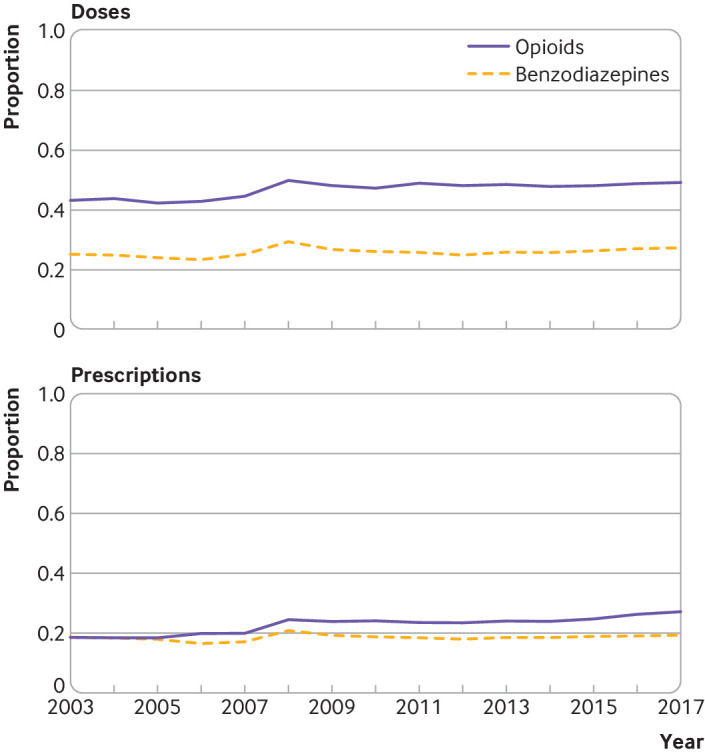
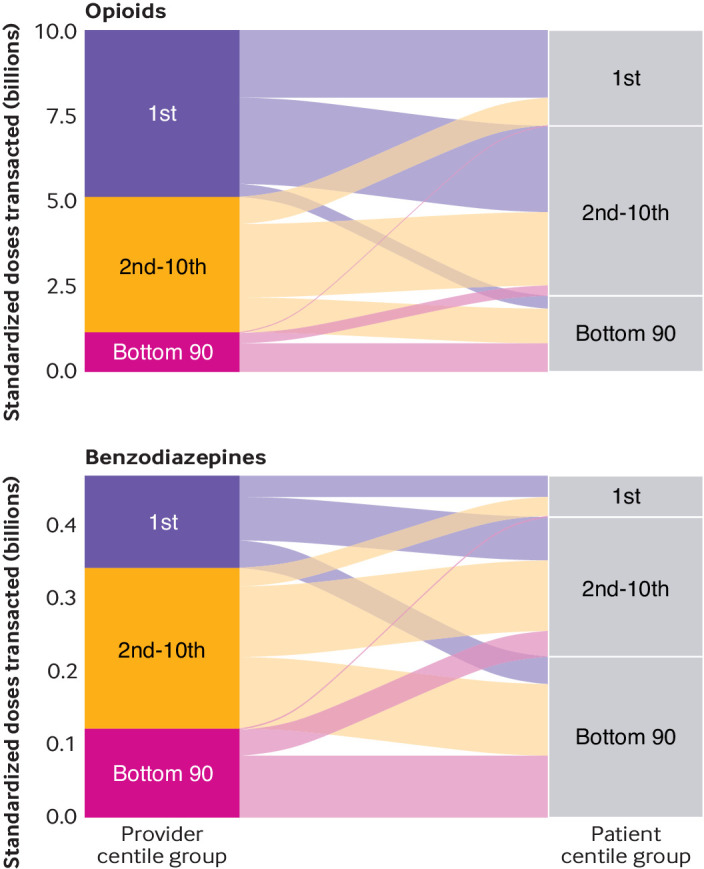
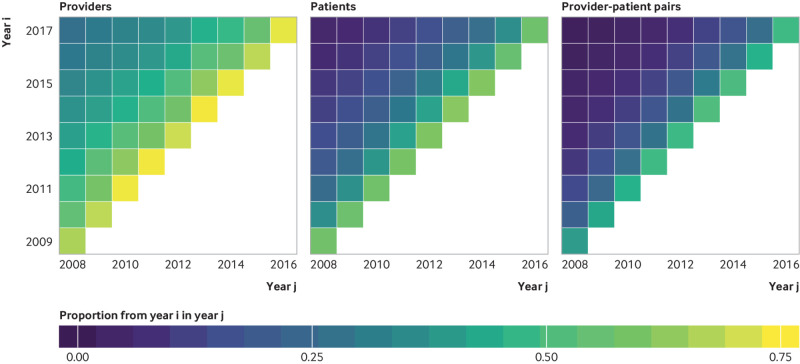
Results: In 2017, the top 1% of providers accounted for 49% of all opioid doses and 27% of all opioid prescriptions. In absolute terms, the top 1% of providers prescribed an average of 748 000 MMEs-nearly 1000 times more than the middle 1%. At least half of all providers in the top 1% in one year were also in the top 1% in adjacent years. More than two fifths of all prescriptions written by the top 1% of providers were for more than 50 MMEs a day and over four fifths were for longer than seven days. In contrast, prescriptions written by the bottom 99% of providers were below these thresholds, with 86% of prescriptions for less than 50 MMEs a day and 71% for fewer than seven days. Providers prescribing high amounts of opioids and patients receiving high amounts of opioids persisted over time, with over half of both appearing in adjacent years.
Conclusions: Most prescriptions written by the majority of providers are under the recommended thresholds, suggesting that most US providers are careful in their prescribing. Interventions focusing on this group of providers are unlikely to effect beneficial change and could induce unnecessary burden. A large proportion of providers have established relationships with their patients over multiple years. Interventions to reduce inappropriate opioid prescribing should be focused on improving patient care, management of patients with complex pain, and reducing comorbidities rather than seeking to enforce a threshold for prescribing.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organization for the submitted work; SB reports grants from the US National Institutes of Health, US Department of Agriculture, and Robert Wood Johnson Foundation, and personal fees from Collective Health, KPMG, Research Triangle International, PLOS Medicine, and the New England Journal of Medicine, outside the submitted work; no financial relationships with any organizations that might have an interested in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Centers for Disease Control and Prevention Vital Signs: Overdoses of Prescription Opioid Pain Relievers---United States, 1999--2008. MMWR Morb Mortal Wkly Rep 2011;60:1487-92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources