

Pragmatic randomised controlled trial of very early etanercept and MTX versus MTX with delayed etanercept in RA: the VEDERA trial
- PMID: 31996367
- PMCID: PMC7147179
- DOI: 10.1136/annrheumdis-2019-216539
Pragmatic randomised controlled trial of very early etanercept and MTX versus MTX with delayed etanercept in RA: the VEDERA trial
Erratum in
-
Correction: Pragmatic randomised controlled trial of very early etanercept and MTX versus MTX with delayed etanercept in RA: the VEDERA trial.Ann Rheum Dis. 2021 Mar;80(3):e45. doi: 10.1136/annrheumdis-2019-216539corr1. Ann Rheum Dis. 2021. PMID: 35737743 Free PMC article. No abstract available.
Abstract
Objectives: We sought to confirm in very early rheumatoid arthritis (ERA) a much greater superiority (30%) of first-line etanercept+methotrexate (ETN+MTX) over treat-to-target MTX (MTX-TT) than previously reported in ERA (14%); and explore whether ETN following initial MTX secures a comparable response to first-line ETN+MTX.
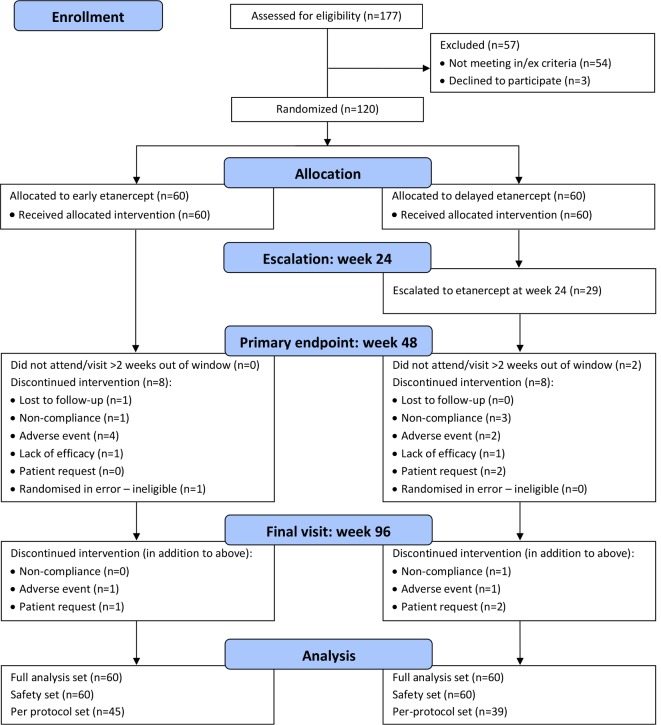
Methods: Pragmatic, open-label, randomised controlled trial of treatment-naïve ERA (≤12 months symptom), Disease Activity Score 28 joint (DAS28)-erythrocyte sedimentation rate (ESR) ≥3.2, rheumatoid factor (RF)+/-anticitrullinated peptide antibody (ACPA) positive or ultrasound power Doppler (PD) if RF and ACPA negative. Subjects were randomised 1:1 to ETN+MTX; or MTX-TT, escalated to ETN if week 24 DAS28-ESR ≥2.6 and intramuscular corticosteroid at protocolised time points. Primary endpoint of week 48 DAS28ESR remission with clinical and imaging secondary endpoints.
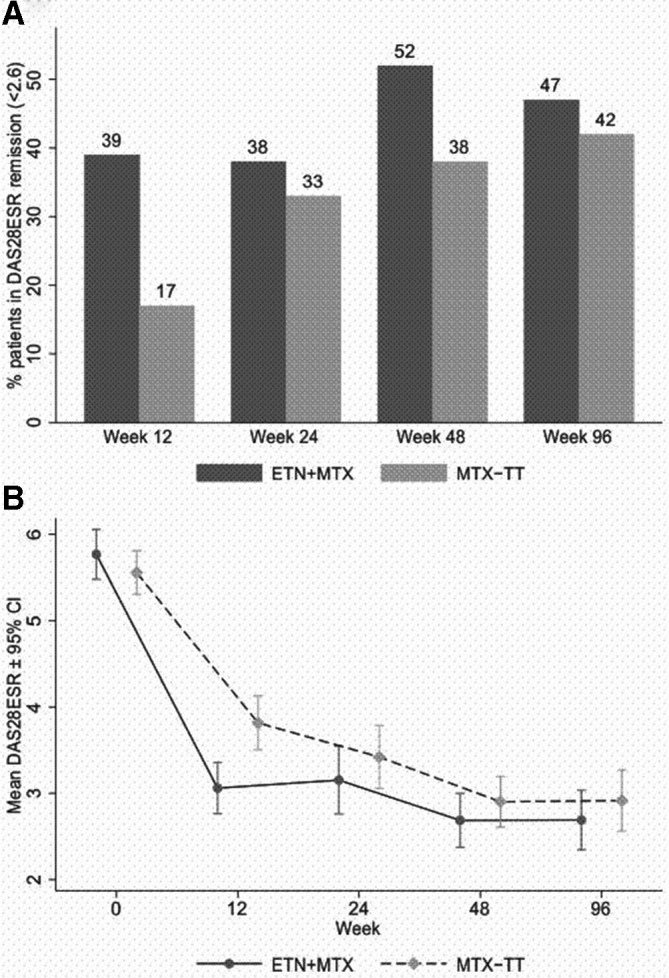
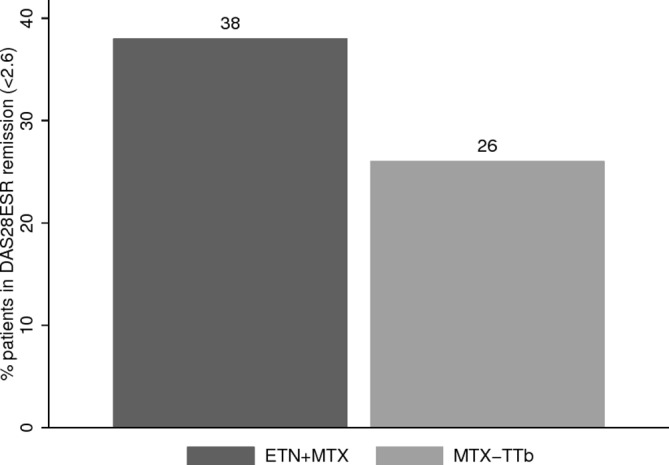
Results: We randomised 120 patients, 60 to each arm (71% female, 73% RF/84% ACPA positive, median (IQR) symptom duration 20.3 (13.1, 30.8) weeks; mean (SD) DAS28 5.1 (1.1)). Remission rates with ETN+MTX and MTX-TT, respectively, were 38% vs 33% at week 24; 52% vs 38% at week 48 (ORs 1.6, 95% CI 0.8 to 3.5, p=0.211). Greater, sustained DAS28-ESR remission observed with ETN+MTX versus MTX-TT (42% and 27%, respectively; p=0.035). PD was fully suppressed by week 48 in over 90% in each arm. Planned exploratory analysis revealed OR 2.84, 95% CI 0.8 to 9.6) of achieving remission after 24 weeks of ETN administered first line compared with administered post-MTX.
Conclusions: Compared with remission rates typically reported with first-line tumour necrosis factor inhabitor+MTX versus MTX-TT, we did not demonstrate a larger effect in very ERA. Neither strategy conferred remission in the majority of patients although ultrasound confirmed local inflammation suppression. Poorer ETN response following failure of MTX-TT is also suggested. Trial registration number NCT02433184.
Keywords: anti-TNF; early rheumatoid arthritis; etanercept; remission; ultrasound.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: PE has undertaken clinical trials and provided expert advice to Pfizer, MSD, Abbvie, BMS, UCB, Roche, Novartis, Samsung, Sandoz and Lilly. PE has received consultant fees from BMS, AbbVie, Pfizer, MSD, Novartis, Roche and UCB. PE has received research grants paid to his employer from AbbVie, BMS, Pfizer, MSD and Roche. MHB has provided expert advice and received consultant fees from AbbVie, Bristol-Myers Squibb, Eli Lilly, EMD Serono, Pfizer, Roche, Sandoz, Sanofi and UCB and has received research grants paid to her employer from Pfizer Bristol-Myers Squibb Ltd, Roche, UCB. DvdH has provided expert advice and received consultant fees from Abbvie, Amgen, Astellas, AstraZeneca, Bristol-Myers Squibb, Boehringer Ingleheim, Celgene, Cyxone, Daichii, Eisai, Eli Lilly, Galapagos, Gilead, GSK, Janssen, Merck, Novartis, Pfizer, Regeneron, Roche, Sanofi, Takeda, UCB Pharma.
Figures
References
-
- Nam JL, Takase-Minegishi K, Ramiro S, et al. Efficacy of biological disease-modifying antirheumatic drugs: a systematic literature review Informing the 2016 update of the EULAR recommendations for the management of rheumatoid arthritis. Ann Rheum Dis 2017;76:1113–36. 10.1136/annrheumdis-2016-210713 - DOI - PubMed
-
- Nam JL, Villeneuve E, Hensor EMA, et al. Remission induction comparing infliximab and high-dose intravenous steroid, followed by treat-to-target: a double-blind, randomised, controlled trial in new-onset, treatment-naive, rheumatoid arthritis (the idea study). Ann Rheum Dis 2014;73:75–85. 10.1136/annrheumdis-2013-203440 - DOI - PubMed
-
- van Vollenhoven RF, Ernestam S, Geborek P, et al. Addition of infliximab compared with addition of sulfasalazine and hydroxychloroquine to methotrexate in patients with early rheumatoid arthritis (Swefot trial): 1-year results of a randomised trial. Lancet 2009;374:459–66. 10.1016/S0140-6736(09)60944-2 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
