

Bolus norepinephrine and phenylephrine for maternal hypotension during elective cesarean section with spinal anesthesia: a randomized, double-blinded study
- PMID: 31996543
- PMCID: PMC7065858
- DOI: 10.1097/CM9.0000000000000621
Bolus norepinephrine and phenylephrine for maternal hypotension during elective cesarean section with spinal anesthesia: a randomized, double-blinded study
Abstract
Background: In recent years, norepinephrine has attracted increasing attention for the management of maternal hypotension during elective cesarean section with spinal anesthesia. Intermittent bolus is a widely used administration paradigm for vasopressors in obstetric anesthesia in China. Thus, in this randomized, double-blinded study, we compared the efficacy and safety of equivalent bolus norepinephrine and phenylephrine for rescuing maternal post-spinal hypotension.
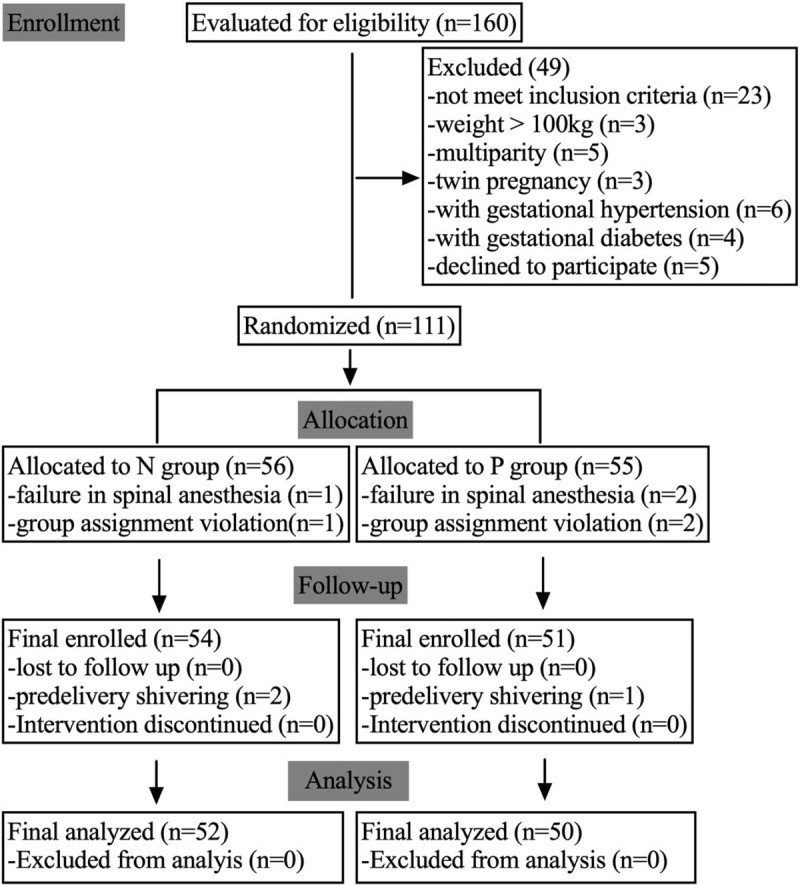
Methods: In a tertiary women's hospital in Nanjing, China, 102 women were allocated with computer derived randomized number to receive prophylactic 8 μg norepinephrine (group N; n = 52) or 100 μg phenylephrine (group P; n = 50) immediately post-spinal anesthesia, followed by an extra bolus of the same dosage until delivery whenever maternal systolic blood pressure became lower than 80% of the baseline. Our primary outcome was standardized maternal cardiac output (CO) reading from spinal anesthesia until delivery analyzed by a two-step method. Other hemodynamic parameters related to vasopressor efficacy and safety were considered as secondary outcomes. Maternal side effects and neonatal outcomes were collected as well.
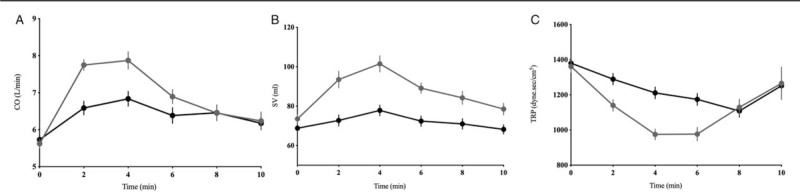
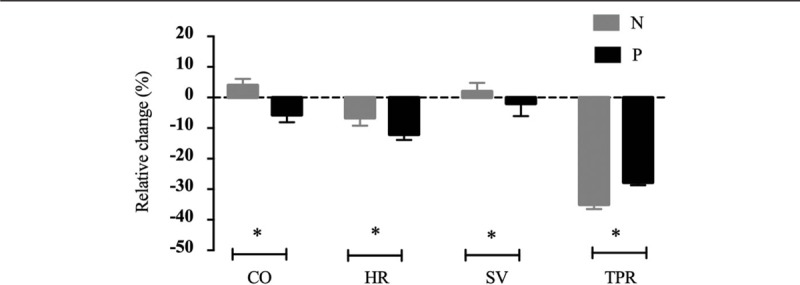
Results: Compared to group P, women in group N had a higher CO (standardized CO 5.8 ± 0.9 vs. 5.3 ± 1.0 L/min, t = 2.37, P = 0.02) and stroke volume (SV, standardized SV 73.6 ± 17.2 vs. 60.0 ± 13.3 mL, t = 4.52, P < 0.001), and a lower total peripheral resistance (875 ± 174 vs. 996 ± 182 dyne·s/cm, t = 3.44, P < 0.001). Furthermore, the incidence of bradycardia was lower in group N than in group P (2% vs. 14%, P = 0.023), along with an overall higher standardized heart rate (78.8 ± 11.6 vs. 75.0 ± 7.3 beats/min, P = 0.049). Other hemodynamics, as well as maternal side effects and neonatal outcomes, were similar in two groups (P > 0.05).
Conclusions: Compared to equivalent phenylephrine, intermittent bolus norepinephrine provides a greater CO for management of maternal hypotension during elective cesarean section with spinal anesthesia; however, no obvious maternal or neonatal clinical advantages were observed for norepinephrine.
Conflict of interest statement
None.
Figures
References
-
- Macarthur A, Riley E. Obstetric anesthesia controversies: vasopressor choice for postspinal hypotension during cesarean delivery. Int Anesthesiol Clin 2007; 45:115–132. doi: 10.1097/AIA.0b013e31802b8d53. - PubMed
-
- Xu S, Shen X, Liu S, Yang J, Wang X. Efficacy and safety of norepinephrine versus phenylephrine for the management of maternal hypotension during cesarean delivery with spinal anesthesia: a systematic review and meta-analysis. Medicine 2019; 98:e14331.doi: 10.1097/MD.0000000000014331. - PMC - PubMed
-
- Kinsella SM, Carvalho B, Dyer RA, Fernando R, Mcdonnell N, Mercier FJ, et al. International consensus statement on the management of hypotension with vasopressors during caesarean section under spinal anaesthesia. Anaesthesia 2018; 73:71–92. doi: 10.1111/anae.14080. - PubMed
-
- Allen TK, Muir HA, George RB, Habib AS. A survey of the management of spinal-induced hypotension for scheduled cesarean delivery. Int J Obstet Anesth 2009; 18:356–361. doi: 10.1016/j.ijoa.2009.03.014. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
