

Non-invasive estimation of cerebral perfusion pressure using transcranial Doppler ultrasonography in children with severe traumatic brain injury
- PMID: 31996979
- PMCID: PMC7223617
- DOI: 10.1007/s00381-020-04524-7
Non-invasive estimation of cerebral perfusion pressure using transcranial Doppler ultrasonography in children with severe traumatic brain injury
Abstract
Objective: To identify if cerebral perfusion pressure (CPP) can be non-invasively estimated by either of two methods calculated using transcranial Doppler ultrasound (TCD) parameters.
Design: Retrospective review of previously prospectively gathered data.
Setting: Pediatric intensive care unit in a tertiary care referral hospital.
Patients: Twenty-three children with severe traumatic brain injury (TBI) and invasive intracranial pressure (ICP) monitoring in place.
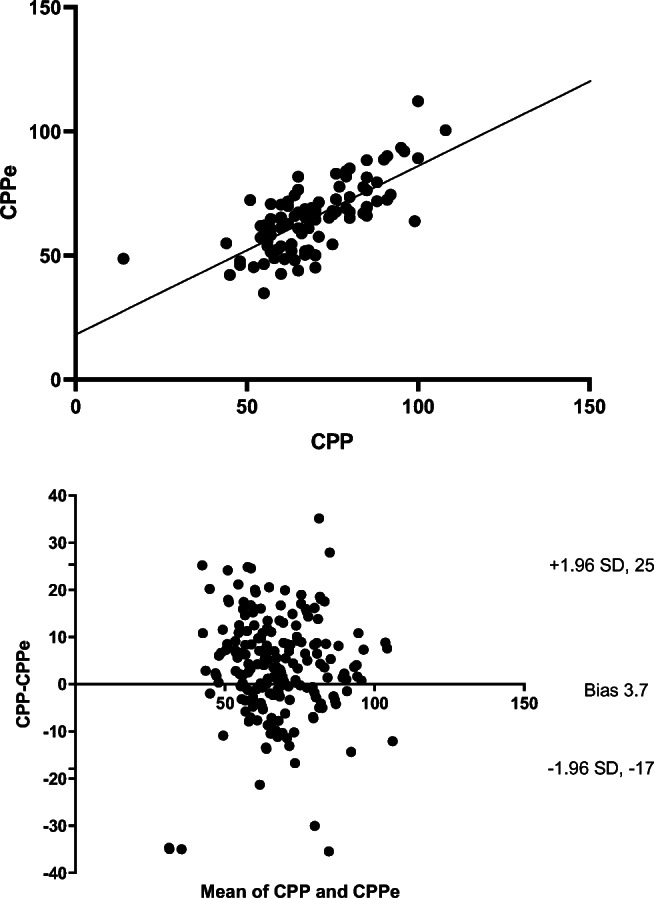
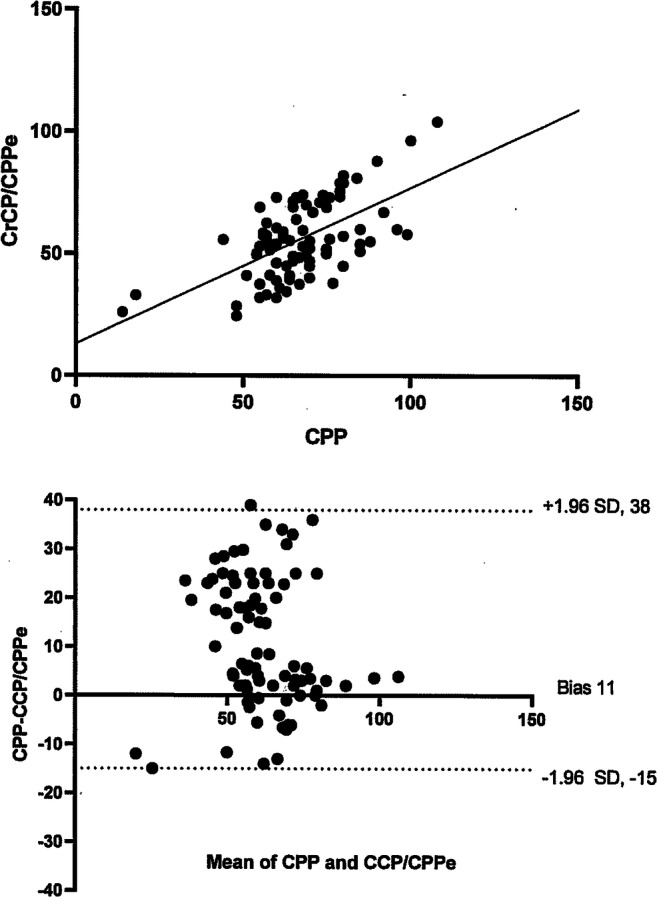
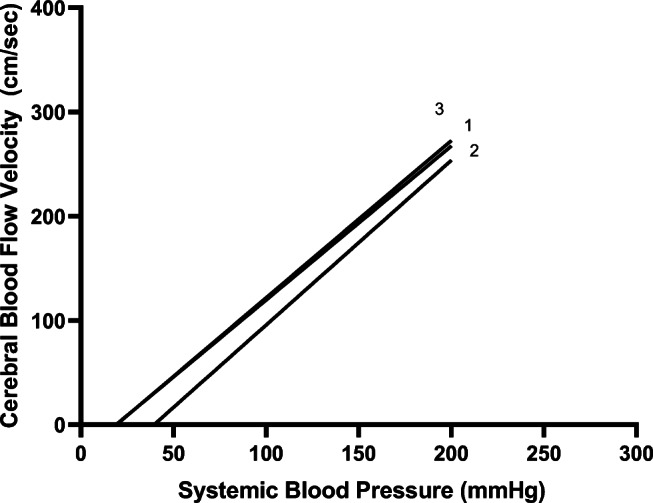
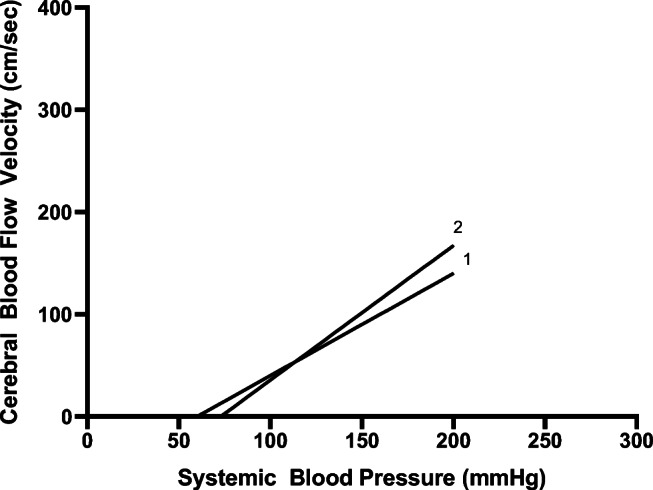
Interventions: TCD evaluation of the middle cerebral arteries was performed daily. CPP at the time of the TCD examination was recorded. For method 1, estimated cerebral perfusion pressure (CPPe) was calculated as: CPPe = MAP × (diastolic flow (Vd)/mean flow (Vm)) + 14. For method 2, critical closing pressure (CrCP) was identified as the intercept point on the x-axis of the linear regression line of blood pressure and flow velocity parameters. CrCP/CPPe was then calculated as MAP-CrCP.
Measurements and main results: One hundred eight paired measurements were available. Using patient averaged data, correlation between CPP and CPPe was significant (r = 0.78, p = < 0.001). However, on Bland-Altman plots, bias was 3.7 mmHg with 95% limits of agreement of - 17 to + 25 for CPPe. Using patient averaged data, correlation between CPP and CrCP/CPPe was significant (r = 0.59, p = < 0.001), but again bias was high at 11 mmHg with wide 95% limits of agreement of - 15 to + 38 mmHg.
Conclusions: CPPe and CrCP/CPPe do not have clinical value to estimate the absolute CPP in pediatric patients with TBI.
Keywords: Cerebral perfusion pressure; Head injury; Non-invasive monitoring; Transcranial Doppler ultrasound; Traumatic brain injury; Ultrasound.
Figures
References
-
- Strauss G, Hansen BA, Kirkgaard P, et al. Liver function, cerebral blood flow autoregulation, and hepatic encephalopathy in fulminant hepatic failure. Hepatology. 1997;25:837–839. - PubMed
-
- Moller K, Larsen FS, Qvist J, et al. Dependency of cerebral blood flow on mean arterial pressure in patients with acute bacterial meningitis. Crit Care Med. 2000;28:1027–1032. - PubMed
-
- Moller K, Qvist T, Tofteng F, et al. Cerebral blood flow and metabolism during infusion of norepinephrine and propofol in patients with bacterial meningitis. Stroke. 2004;35:1333–1339. - PubMed
-
- Newell DW, Aaslid R, Lam A, Mayberg TS, Winn HR. Comparison of flow and velocity during dynamic autoregulation testing in humans. Stroke. 1994;25:793–797. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
