

Highlights in heart failure
- PMID: 31997538
- PMCID: PMC6989277
- DOI: 10.1002/ehf2.12555
Highlights in heart failure
Abstract
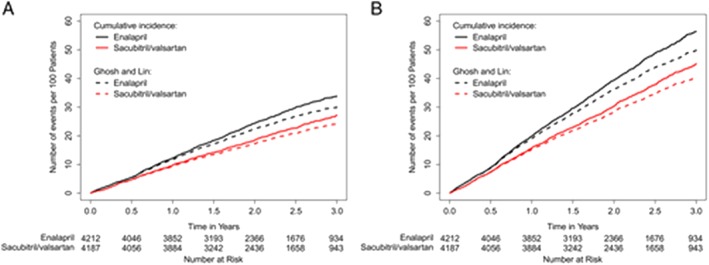
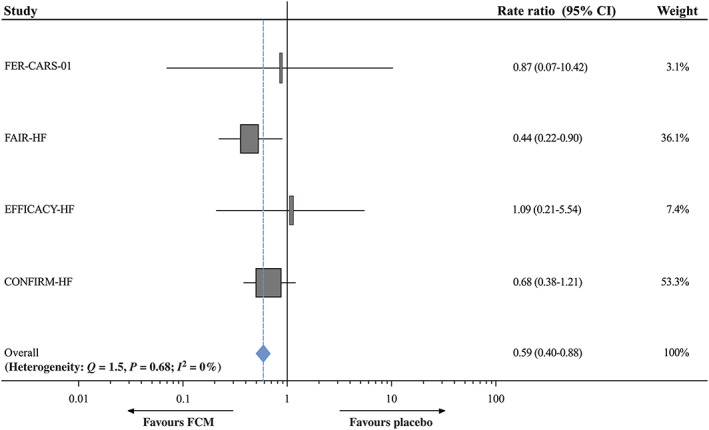
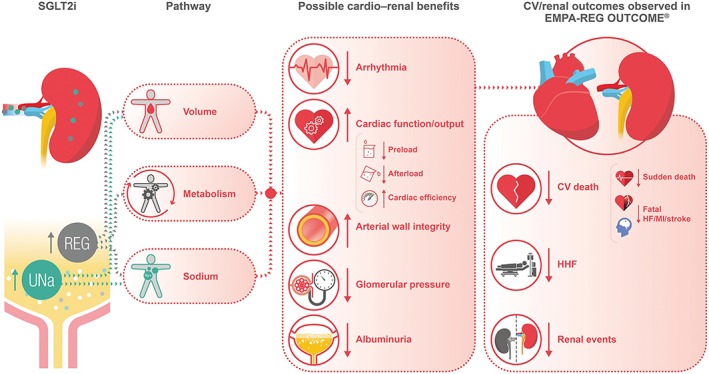
Heart failure (HF) remains a major cause of mortality, morbidity, and poor quality of life. It is an area of active research. This article is aimed to give an update on recent advances in all aspects of this syndrome. Major changes occurred in drug treatment of HF with reduced ejection fraction (HFrEF). Sacubitril/valsartan is indicated as a substitute to ACEi/ARBs after PARADIGM-HF (hazard ratio [HR], 0.80; 95% confidence interval [CI], 0.73 to 0.87 for sacubitril/valsartan vs. enalapril for the primary endpoint and Wei, Lin and Weissfeld HR 0.79, 95% CI 0.71-0.89 for recurrent events). Its initiation was then shown as safe and potentially useful in recent studies in patients hospitalized for acute HF. More recently, dapagliflozin and prevention of adverse-outcomes in DAPA-HF trial showed the beneficial effects of the sodium-glucose transporter type 2 inhibitor dapaglifozin vs. placebo, added to optimal standard therapy [HR, 0.74; 95% CI, 0.65 to 0.85;0.74; 95% CI, 0.65 to 0.85 for the primary endpoint]. Trials with other SGLT 2 inhibitors and in other patients, such as those with HF with preserved ejection fraction (HFpEF) or with recent decompensation, are ongoing. Multiple studies showed the unfavourable prognostic significance of abnormalities in serum potassium levels. Potassium lowering agents may allow initiation and titration of mineralocorticoid antagonists in a larger proportion of patients. Meta-analyses suggest better outcomes with ferric carboxymaltose in patients with iron deficiency. Drugs effective in HFrEF may be useful also in HF with mid-range ejection fraction. Better diagnosis and phenotype characterization seem warranted in HF with preserved ejection fraction. These and other burning aspects of HF research are summarized and reviewed in this article.
Keywords: HFmrEF; HFpEF; HFrEF; acute heart failure; heart failure; treatment.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Figures
References
-
- Cooper LB, Yap J, Tay WT, Teng TK, MacDonald M, Anand IS, Sharma A, O'Connor CM, Kraus WE, Mentz RJ, Lam CS, Hf A, Investigators A‐H. Multi‐ethnic comparisons of diabetes in heart failure with reduced ejection fraction: insights from the HF‐ACTION trial and the ASIAN‐HF registry. Eur J Heart Fail 2018; 20: 1281–1289. - PubMed
-
- Nagai T, Sundaram V, Shoaib A, Shiraishi Y, Kohsaka S, Rothnie KJ, Piper S, McDonagh TA, Hardman SMC, Goda A, Mizuno A, Sawano M, Rigby AS, Quint JK, Yoshikawa T, Clark AL, Anzai T, Cleland JGF. Validation of U.S. mortality prediction models for hospitalized heart failure in the United Kingdom and Japan. Eur J Heart Fail 2018; 20: 1179–1190. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, Gonzalez‐Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, Authors/Task Force M and Document R . 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2016; 18: 891–975. - PubMed
-
- Komajda M, Bohm M, Borer JS, Ford I, Tavazzi L, Pannaux M, Swedberg K. Incremental benefit of drug therapies for chronic heart failure with reduced ejection fraction: a network meta‐analysis. Eur J Heart Fail 2018; 20: 1315–1322. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
