

Performance of F-18 Fluorocholine PET/CT for Detection of Hyperfunctioning Parathyroid Tissue in Patients with Elevated Parathyroid Hormone Levels and Negative or Discrepant Results in conventional Imaging
- PMID: 31997599
- PMCID: PMC6992441
- DOI: 10.3348/kjr.2019.0268
Performance of F-18 Fluorocholine PET/CT for Detection of Hyperfunctioning Parathyroid Tissue in Patients with Elevated Parathyroid Hormone Levels and Negative or Discrepant Results in conventional Imaging
Abstract
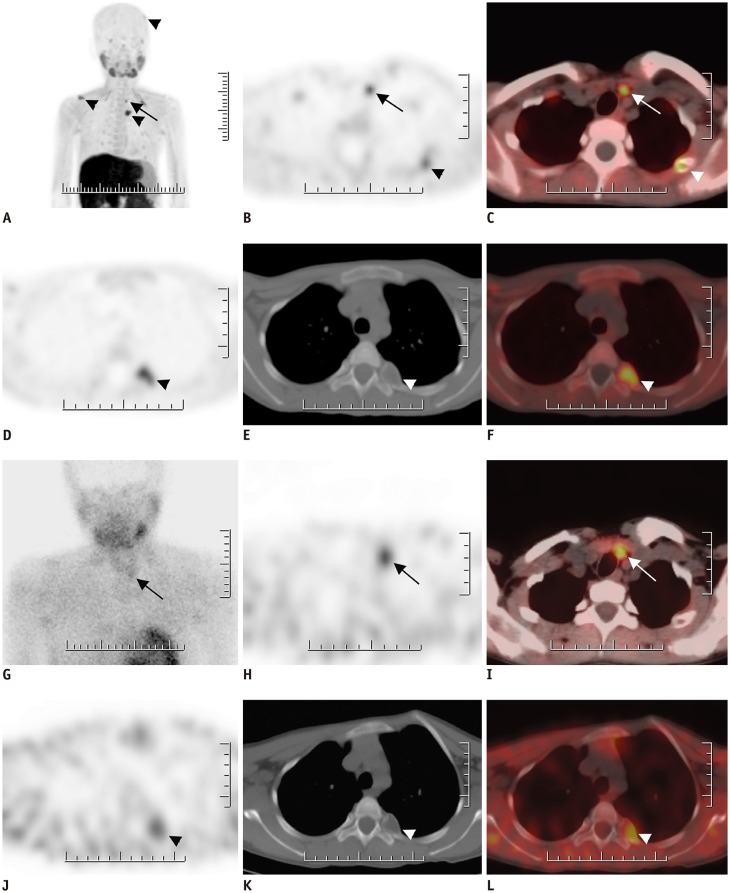
Objective: Our aim was to assess the diagnostic performance of F-18 fluorocholine (FCH) positron emission tomography/computed tomography (PET/CT) in detecting hyperfunctioning parathyroid tissue (HPT) in patients with elevated parathyroid hormone levels with negative or inconclusive conventional imaging results and to compare the findings with those obtained using technetium-99m sestamibi (MIBI) scintigraphy and neck ultrasonography (US).
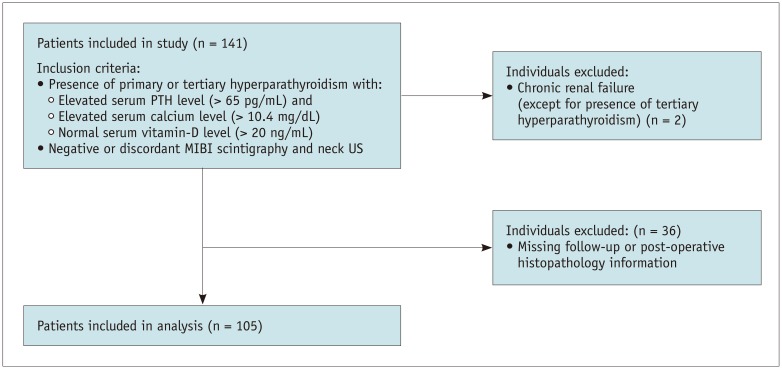
Materials and methods: Images of 105 patients with hyperparathyroidism who underwent FCH PET/CT, dual-phase MIBI parathyroid scintigraphy (median interval: 42 days), and neck US were retrospectively analyzed. The gold standard was histopathological findings for 81 patients who underwent parathyroidectomy and clinical follow-up findings in the remaining 24 patients. Sensitivities, positive predictive values (PPVs), and accuracies were calculated for all imaging modalities.
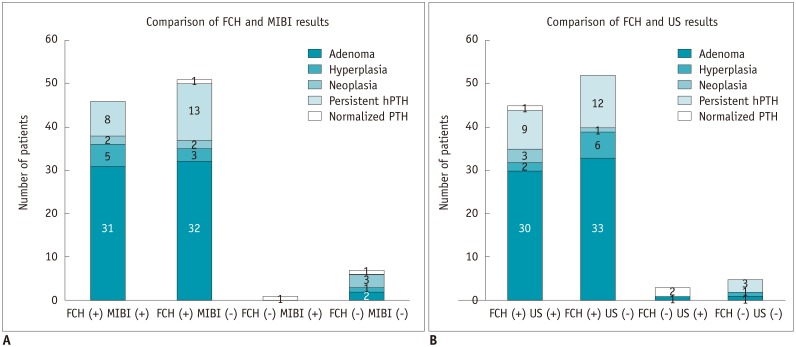
Results: Among the 81 patients who underwent parathyroidectomy, either parathyroid adenoma (n = 64), hyperplasia (n = 9), neoplasia (n = 4), or both parathyroid adenoma and hyperplasia (n = 1) were detected, except 3 patients who did not show HPT. Of the 24 (23%) patients who were followed-up without operation, 22 (92%) showed persistent hyperparathyroidism. FCH PET/CT showed significantly higher sensitivity than MIBI scintigraphy and US in detection of HPT (p < 0.01). Sensitivity, PPV, and accuracy of FCH PET/CT were 94.1% (95/101), 97.9% (95/97), and 92.4% (97/105), respectively. The corresponding values for MIBI scintigraphy and US were 45.1% (46/102), 97.9% (46/47), and 45.7% (48/105) and 44.1% (45/102), 93.8% (45/48), and 42.9% (45/105), respectively. Among the 35 patients showing negative MIBI scintigraphy and neck US findings, 30 (86%) showed positive results on FCH PET/CT. FCH PET/CT could demonstrate ectopic locations of HPT in 11 patients whereas MIBI and US showed positive findings in only 6 and 3 patients, respectively.
Conclusion: FCH PET/CT is an effective imaging modality for detection of HPT with the highest sensitivity among the available imaging techniques. Therefore, FCH PET/CT can be recommended especially for patients who show negative or inconclusive results on conventional imaging.
Keywords: Computed tomography; Fluorocholine; Hyperparathyroidism; Parathyroid adenoma; Positron emission tomography; Tc-99m sestamibi.
Copyright © 2020 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Wilhelm SM, Wang TS, Ruan DT, Lee JA, Asa SL, Duh QY, et al. The American Association of Endocrine Surgeons guidelines for definitive management of primary hyperparathyroidism. JAMA Surg. 2016;151:959–968. - PubMed
-
- Ciappuccini R, Morera J, Pascal P, Rame JP, Heutte N, Aide N, et al. Dual-phase 99mTc sestamibi scintigraphy with neck and thorax SPECT/CT in primary hyperparathyroidism: a single-institution experience. Clin Nucl Med. 2012;37:223–228. - PubMed
-
- Hunter GJ, Schellingerhout D, Vu TH, Perrier ND, Hamberg LM. Accuracy of four-dimensional CT for the localization of abnormal parathyroid glands in patients with primary hyperparathyroidism. Radiology. 2012;264:789–795. - PubMed
-
- Mahajan A, Starker LF, Ghita M, Udelsman R, Brink JA, Carling T. Parathyroid four-dimensional computed tomography: evaluation of radiation dose exposure during preoperative localization of parathyroid tumors in primary hyperparathyroidism. World J Surg. 2012;36:1335–1339. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
