

Pilot Study of Hyperfractionated Dosing of Lutetium-177-Labeled Antiprostate-Specific Membrane Antigen Monoclonal Antibody J591 (177 Lu-J591) for Metastatic Castration-Resistant Prostate Cancer
- PMID: 31999003
- PMCID: PMC7288642
- DOI: 10.1634/theoncologist.2020-0028
Pilot Study of Hyperfractionated Dosing of Lutetium-177-Labeled Antiprostate-Specific Membrane Antigen Monoclonal Antibody J591 (177 Lu-J591) for Metastatic Castration-Resistant Prostate Cancer
Abstract
Lessons learned: Hyperfractionation of lutetium-177 (177 Lu)-J591 for patients with metastatic castration-resistant prostate cancer did not appear to have any additional advantage over the single dose 177 Lu-J591 or fractionated two-dose 177 Lu-J591 therapy. Definite conclusions were challenging because of the small sample size of this study, and so further studies are needed to evaluate the viability of the hypothesis. On the basis of available data, a registration study of 177 Lu-J591 (also known as TLX591) is planned and will use the two-dose fractionation schedule (Telix Pharma Q3 2019 update https://telixpharma.com/news-media/).
Background: Phase I and II single-dose studies of lutetium-177 (177 Lu)-J591, a radio-labeled antibody binding prostate-specific membrane antigen (PSMA), demonstrated safety and efficacy with dose response. Modest dose fractionation of 177 Lu-J591 (2 doses) has less myelosuppression per similar cumulative dose, allowing higher doses to be administered safely. We hypothesized that additional dose fractionation would allow a higher cumulative dose, potentially with less toxicity and more efficacy.
Methods: Men with progressive metastatic castration-resistant prostate cancer and adequate organ function were enrolled. 177 Lu-J591 was administered at 25 mCi/m2 every 2 weeks until the emergence of related grade 2 toxicity. 177 Lu-J591 imaging was performed and circulating tumor cell (CTC) counts were measured before and after treatment along with standard monitoring.
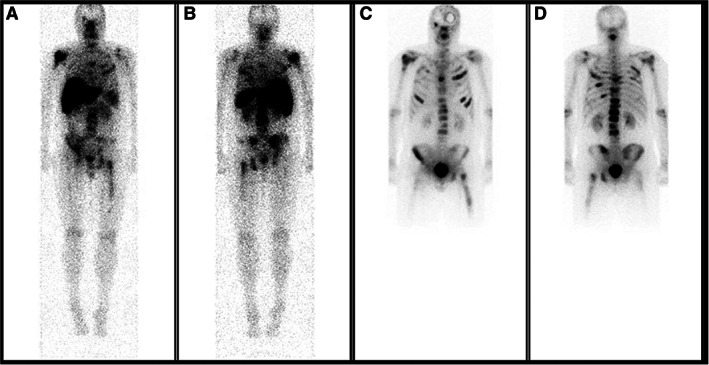
Results: Six subjects in a single cohort, with a median age of 68.6 years, were enrolled. Patients received three to six doses (cumulative 75-150 mCi/m2 ). Two (33%) patients had >30% prostate-specific antigen (PSA) decline and three (50%) had CTC count decline. Two (33%) experienced grade (Gr) 4 neutropenia (without fever), three (50%) had Gr 4 thrombocytopenia (without hemorrhage), and two (33%) required platelet transfusions. Following hematological improvement, two patients developed worsening cytopenia during prostate cancer progression; bone marrow biopsies revealed infiltrative tumor replacing normal marrow elements without myelodysplasia. Targeting of known disease sites was seen on planar imaging in all.
Conclusion: Hyperfractionation of 177 Lu-J591 is feasible but does not seem to have significant advantages over the two-dose fractionation regimen.
© AlphaMed Press; the data published online to support this summary are the property of the authors.
Figures
References
-
- Bostwick DG, Pacelli A, Blute M et al. Prostate specific membrane antigen expression in prostatic intraepithelial neoplasia and adenocarcinoma: A study of 184 cases. Cancer 1998;82:2256–2261. - PubMed
-
- Bander NH, Nanus DM, Milowsky MI et al. Targeted systemic therapy of prostate cancer with a monoclonal antibody to prostate‐specific membrane antigen. Semin Oncol 2003;30:667–676. - PubMed
-
- Bander NH, Milowsky MI, Nanus DM et al. Phase I trial of 177lutetium‐labeled J591, a monoclonal antibody to prostate‐specific membrane antigen, in patients with androgen‐independent prostate cancer. J Clin Oncol 2005;23:4591–4601. - PubMed
-
- Tagawa ST, Vallabhajosula S, Christos PJ et al. Phase 1/2 study of fractionated dose lutetium‐177‐labeled anti‐prostate‐specific membrane antigen monoclonal antibody J591 (177Lu‐J591) for metastatic castration‐resistant prostate cancer. Cancer 2019;125:2561–2569. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
