

Early noncardiovascular organ failure and mortality in the cardiac intensive care unit
- PMID: 31999370
- PMCID: PMC7244298
- DOI: 10.1002/clc.23339
Early noncardiovascular organ failure and mortality in the cardiac intensive care unit
Abstract
Background: Noncardiac organ failure has been associated with worse outcomes among a cardiac intensive care unit (CICU) population.
Hypothesis: We hypothesized that early organ failure based on the sequential organ failure assessment (SOFA) score would be associated with mortality in CICU patients.
Methods: Adult CICU patients from 2007 to 2015 were reviewed. Organ failure was defined as any SOFA organ subscore ≥3 on the first CICU day. Organ failure was evaluated as a predictor of hospital mortality and postdischarge survival after adjustment for illness severity and comorbidities.
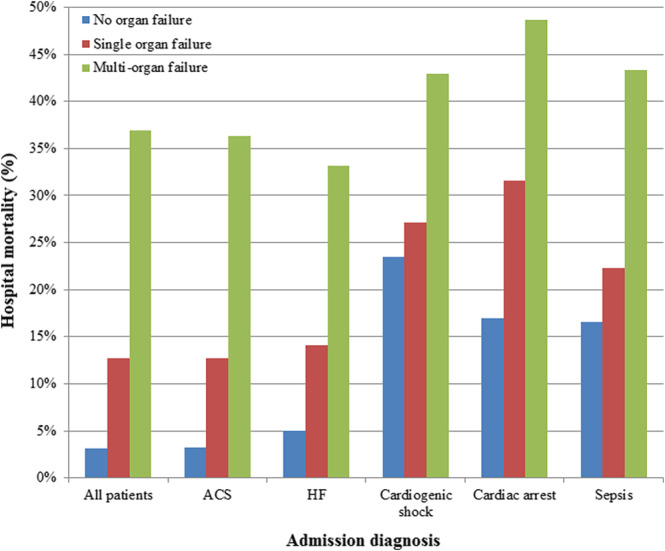
Results: We included 10 004 patients with a mean age of 67 ± 15 years (37% female). Admission diagnoses included acute coronary syndrome in 43%, heart failure in 46%, cardiac arrest in 12%, and cardiogenic shock in 11%. Organ failure was present in 31%, including multiorgan failure in 12%. Hospital mortality was higher in patients with organ failure (22% vs 3%, adjusted OR 3.0, 95% CI 2.5-3.7, P < .001). After adjustment, each failing organ system predicted twofold higher odds of hospital mortality (adjusted OR 1.9, 95% CI 1.1-2.1, P < .001). Mortality risk was highest with cardiovascular, coagulation and liver failure. Among hospital survivors, organ failure was associated with higher adjusted postdischarge mortality risk (P < .001); multiorgan failure did not confer added long-term mortality risk.
Conclusions: Early noncardiovascular organ failure, especially multiorgan failure, is associated with increased hospital mortality in CICU patients, and this risk continues after hospital discharge, emphasizing the need to promote early recognition of organ failure in CICU patients.
Keywords: cardiac critical care; cardiac intensive care unit; mortality; organ failure; sequential organ failure assessment (SOFA) score.
© 2020 The Authors. Clinical Cardiology published by Wiley Periodicals, Inc.
Conflict of interest statement
The authors declare that there are no relevant financial disclosures or conflicts of interest related to this work.
Figures


References
-
- Jentzer JC, van Diepen S, Barsness GW, et al. Changes in comorbidities, diagnoses, therapies and outcomes in a contemporary cardiac intensive care unit population. Am Heart J. 2019;215:12‐19. - PubMed
-
- Katz JN, Shah BR, Volz EM, et al. Evolution of the coronary care unit: clinical characteristics and temporal trends in healthcare delivery and outcomes. Crit Care Med. 2010;38(2):375‐381. - PubMed
-
- Casella G, Cassin M, Chiarella F, et al. Epidemiology and patterns of care of patients admitted to Italian intensive cardiac care units: the BLITZ‐3 registry. J Cardiovasc Med (Hagerstown). 2010;11(6):450‐461. - PubMed
-
- Holland EM, Moss TJ. Acute noncardiovascular illness in the cardiac intensive care unit. J Am Coll Cardiol. 2017;69(16):1999‐2007. - PubMed
-
- Goldfarb M, van Diepen S, Liszkowski M, Jentzer JC, Pedraza I, Cercek B. Noncardiovascular disease and critical care delivery in a contemporary cardiac and medical intensive care unit. J Intensive Care Med. 2017;34(7):537‐543. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
