

Overcoming acquired resistance of epidermal growth factor receptor-mutant non-small cell lung cancer cells to osimertinib by combining osimertinib with the histone deacetylase inhibitor panobinostat (LBH589)
- PMID: 31999837
- PMCID: PMC7241261
- DOI: 10.1002/cncr.32744
Overcoming acquired resistance of epidermal growth factor receptor-mutant non-small cell lung cancer cells to osimertinib by combining osimertinib with the histone deacetylase inhibitor panobinostat (LBH589)
Abstract
Background: The major clinical obstacle that limits the long-term benefits of treatment with osimertinib (AZD9291) in patients with epidermal growth factor receptor-mutant non-small cell lung cancer is the development of acquired resistance. Therefore, effective strategies that can overcome acquired resistance to osimertinib are urgently needed. The authors' current efforts in this direction have identified LBH589 (panobinostat), a clinically used histone deacetylase inhibitor, as a potential agent in overcoming osimertinib resistance.
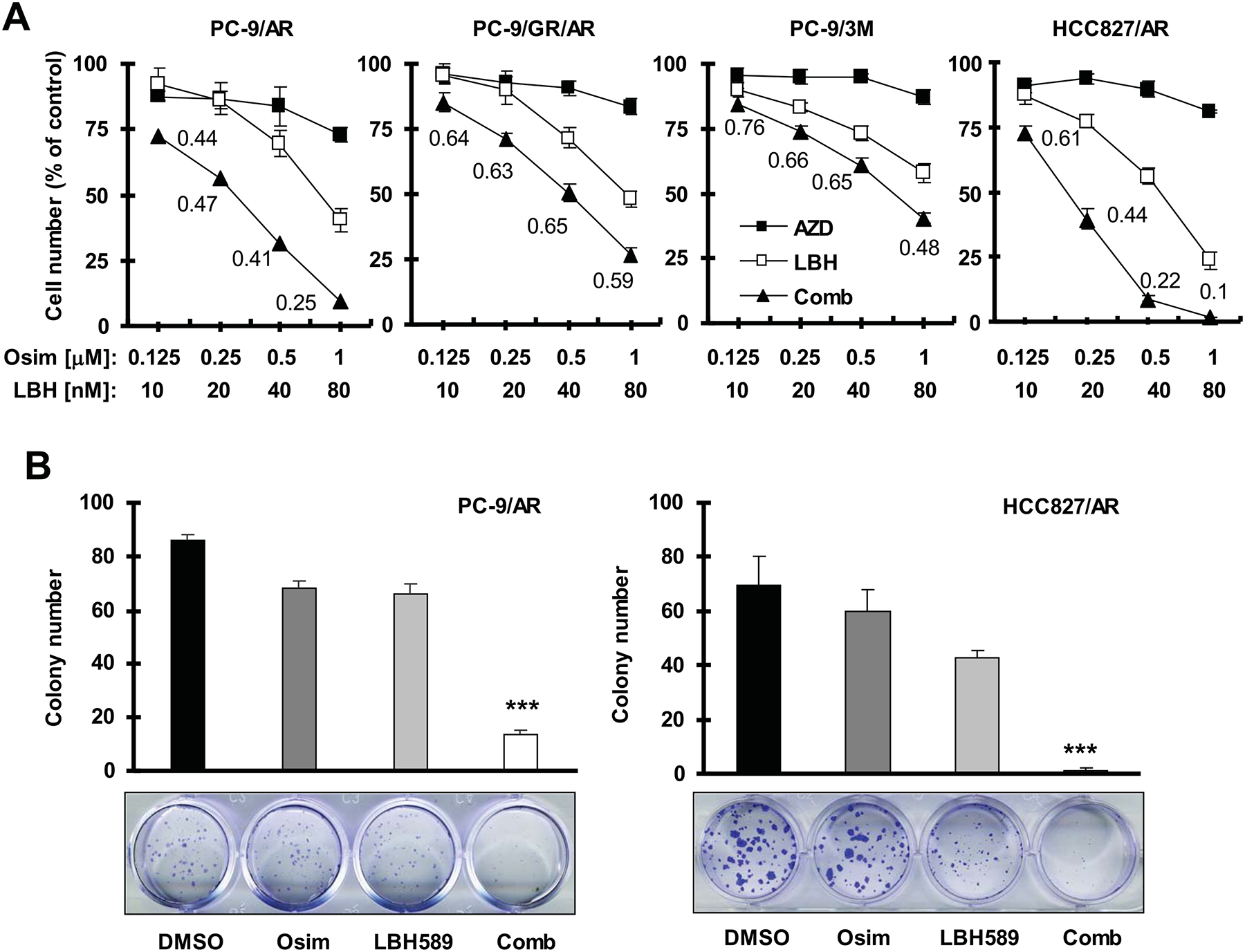
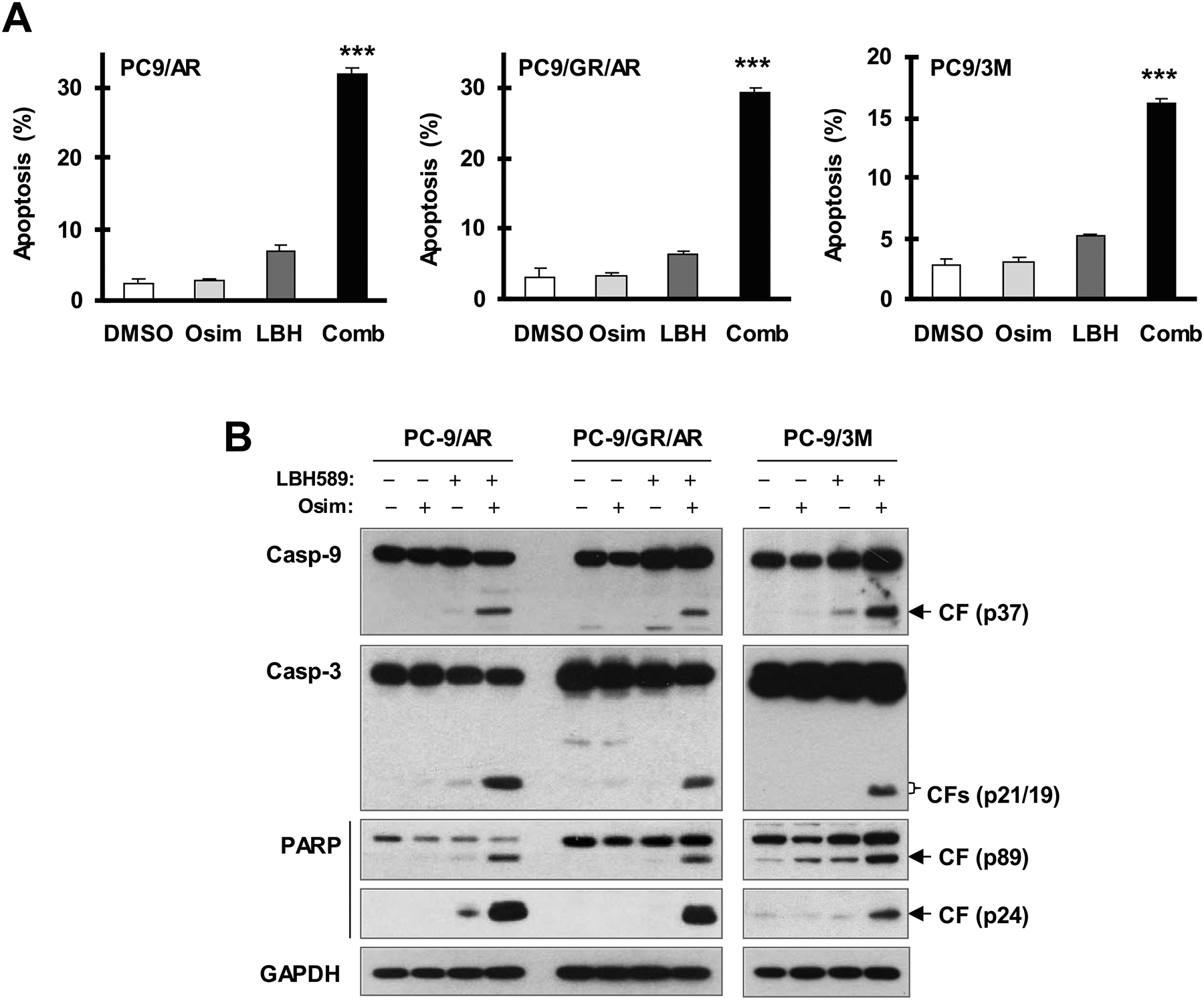
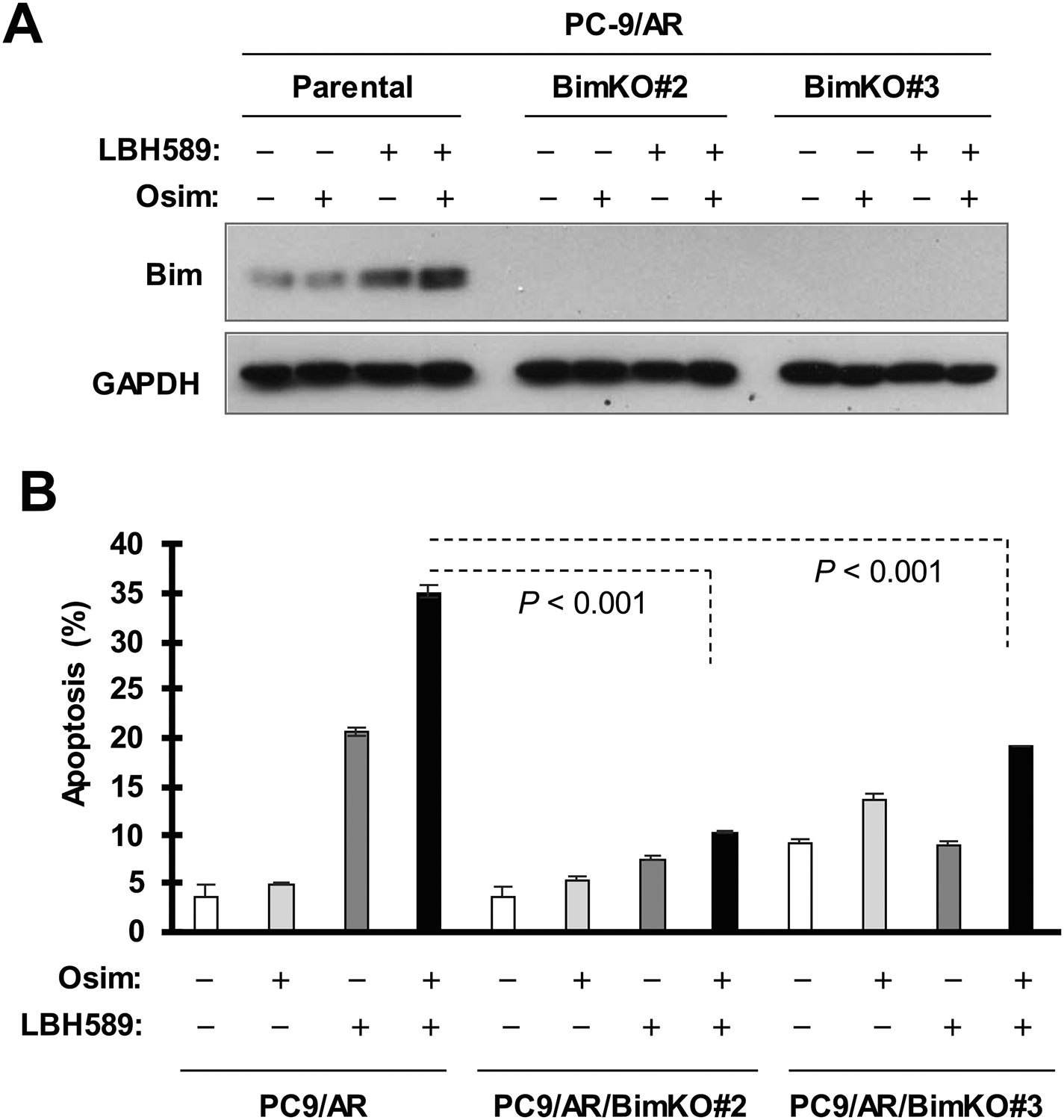
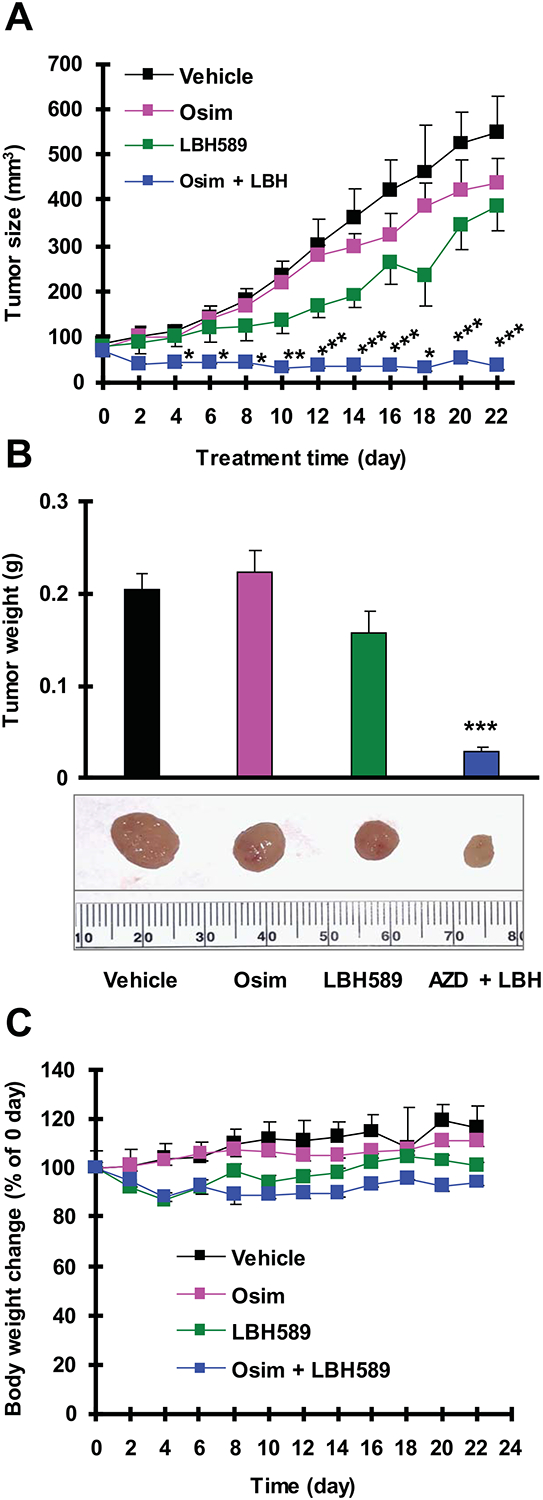
Methods: Cell growth and apoptosis in vitro were evaluated by measuring cell numbers and colony formation and by detecting annexin V-positive cells and protein cleavage, respectively. Drug effects on tumor growth in vivo were assessed with xenografts in nude mice. Alterations of tested proteins in cells were monitored with Western blot analysis. Gene knockout was achieved using the CRISPR/Cas9 technique.
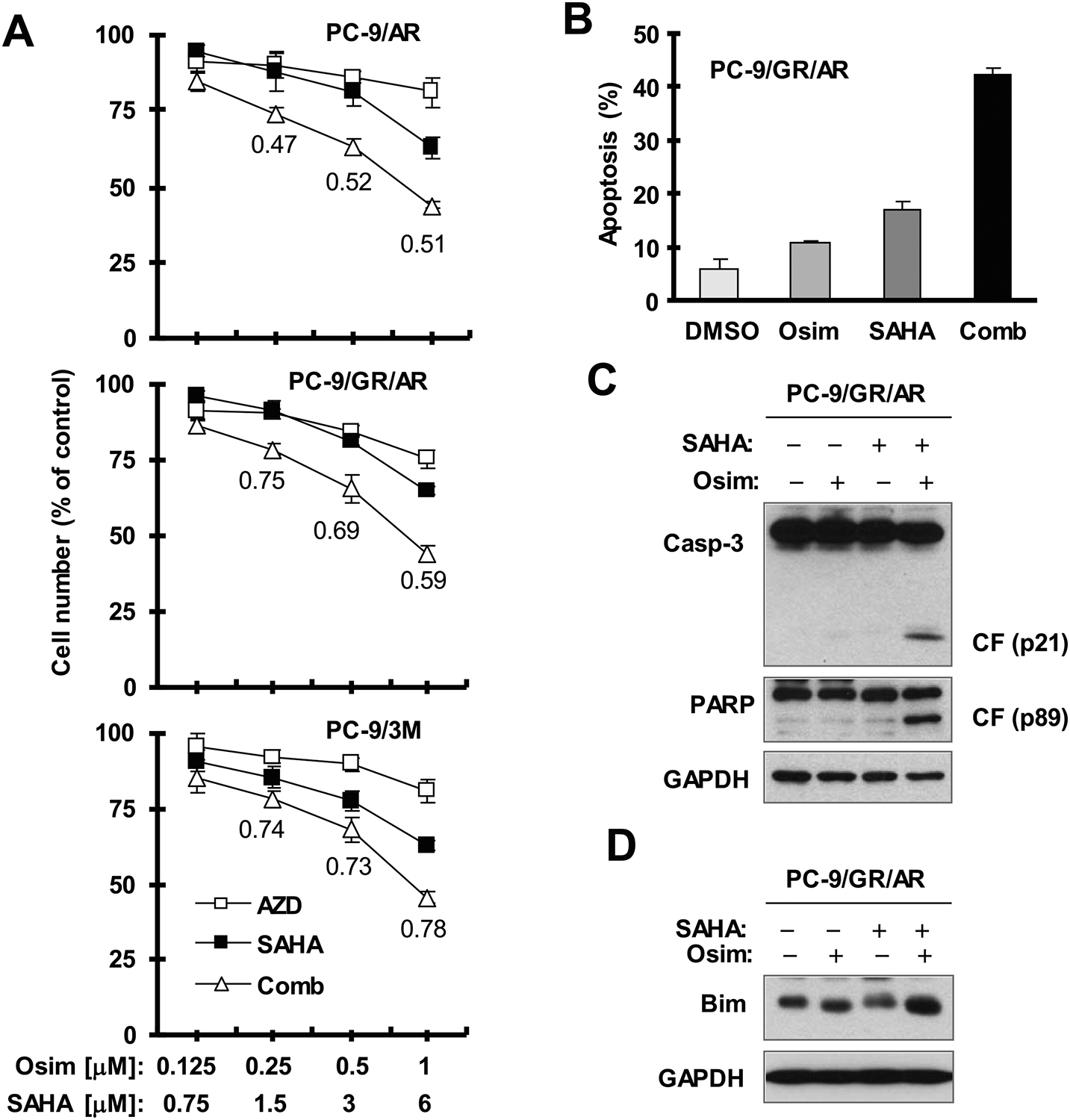
Results: The combination of LBH589 and osimertinib synergistically decreased the survival of different osimertinib-resistant cell lines, including those harboring C797S mutations, with greater inhibition of cell colony formation and growth. The combination enhanced the induction of apoptosis in osimertinib-resistant cells. Importantly, the combination effectively inhibited the growth of osimertinib-resistant xenograft tumors in nude mice. Mechanistically, the combination of LBH589 and osimertinib enhanced the elevation of Bim in osimertinib-resistant cells. Knockout of Bim in osimertinib-resistant cells substantially attenuated or abolished apoptosis enhanced by the LBH589 and osimertinib combination. These results collectively support a critical role of Bim elevation in the induction of apoptosis of osimertinib-resistant cells for this combination.
Conclusions: The current findings provide strong preclinical evidence in support of the potential for LBH589 to overcome osimertinib resistance in the clinic.
Keywords: LBH589; acquired resistance; apoptosis; epidermal growth factor receptor (EGFR); histone deacetylase (HDAC); lung cancer; osimertinib.
© 2020 American Cancer Society.
Conflict of interest statement
Figures

References
-
- Russo A, Franchina T, Ricciardi GRR, et al. Third generation EGFR TKIs in EGFR-mutated NSCLC: Where are we now and where are we going. Crit Rev Oncol Hematol. 2017;117: 38–47. - PubMed
-
- Tartarone A, Lerose R. Clinical approaches to treat patients with non-small cell lung cancer and epidermal growth factor receptor tyrosine kinase inhibitor acquired resistance. Ther Adv Respir Dis. 2015;9: 242–250. - PubMed
-
- Juchum M, Gunther M, Laufer SA. Fighting cancer drug resistance: Opportunities and challenges for mutation-specific EGFR inhibitors. Drug Resist Updat. 2015;20: 10–28. - PubMed
-
- Remon J, Moran T, Majem M, et al. Acquired resistance to epidermal growth factor receptor tyrosine kinase inhibitors in EGFR-mutant non-small cell lung cancer: A new era begins. Cancer Treat Rev. 2014;40: 93–101. - PubMed
-
- Govindan R Overcoming resistance to targeted therapy for lung cancer. N Engl J Med. 2015;372: 1760–1761. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
