

Symptom Experiences in Colorectal Cancer Survivors After Cancer Treatments: A Systematic Review and Meta-analysis
- PMID: 32000174
- PMCID: PMC7182500
- DOI: 10.1097/NCC.0000000000000785
Symptom Experiences in Colorectal Cancer Survivors After Cancer Treatments: A Systematic Review and Meta-analysis
Abstract
Background: With improved survivorship rates for colorectal cancer (CRC), more CRC survivors are living with long-term disease and treatment side effects. Little research exists on CRC symptoms or symptom management guidelines to support these individuals after cancer treatments.
Objectives: The aims of this study were to systematically review symptom experiences, risk factors, and the impact of symptoms and to examine the pooled frequency and severity of symptoms via meta-analyses in CRC survivors after cancer treatments.
Methods: Relevant studies were systematically searched in 7 databases from 2009 to 2019. Meta-analysis was conducted for pooled estimates of symptom frequency and severity.
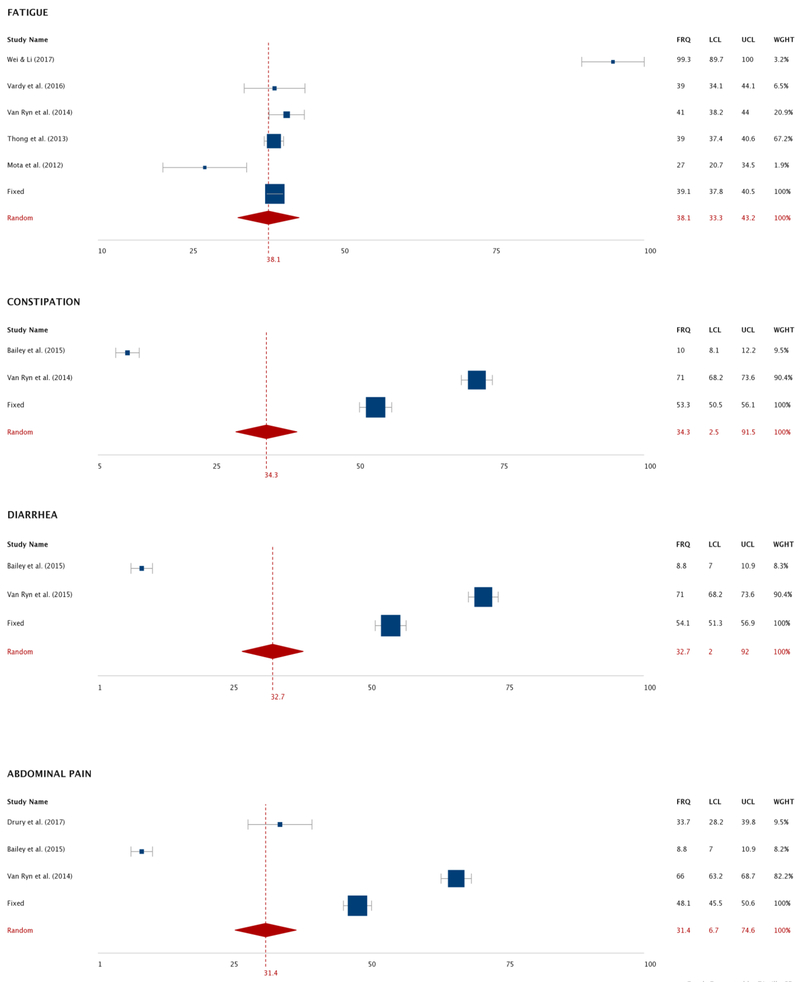
Results: Thirty-five studies met the inclusion criteria. Six studies assessed multiple CRC symptoms, whereas 29 focused on a single symptom, including peripheral neuropathy, psychological distress, fatigue, body image distress, cognitive impairment, and insomnia. The pooled mean frequency was highest for body image distress (78.5%). On a scale of 0 to 100, the pooled mean severity was highest for fatigue (50.1). Gastrointestinal and psychological symptoms, peripheral neuropathy, and insomnia were also major problems in CRC survivors. Multiple factors contributed to adverse symptoms, such as younger age, female gender, and lack of family/social support. Symptoms negatively impacted quality of life, social and sexual functioning, financial status, and caregivers' physical and mental conditions.
Conclusions: Colorectal cancer survivors experienced multiple adverse symptoms related to distinct risk factors. These symptoms negatively impacted patients and caregivers' well-being.
Implications for practice: Healthcare providers can use study findings to better assess and monitor patient symptoms after cancer treatments. More research is needed on CRC-specific symptoms and their effective management.
Conflict of interest statement
Conflict of interest:
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures








References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. - PubMed
-
- Drury A, Payne S, Brady AM. The cost of survival: an exploration of colorectal cancer survivors' experiences of pain. Acta Oncol. 2017;56(2):205–211. - PubMed
-
- Rasmussen S, Larsen PV, Sondergaard J, Elnegaard S, Svendsen RP, Jarbol DE. Specific and non-specific symptoms of colorectal cancer and contact to general practice. Fam Prac. 2015;32(4):387–394. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
