

Time to appropriate antibiotic therapy is a predictor of outcome in patients with bloodstream infection caused by KPC-producing Klebsiella pneumoniae
- PMID: 32000834
- PMCID: PMC6993311
- DOI: 10.1186/s13054-020-2742-9
Time to appropriate antibiotic therapy is a predictor of outcome in patients with bloodstream infection caused by KPC-producing Klebsiella pneumoniae
Abstract
Background: Bloodstream infections (BSIs) by Klebsiella pneumoniae carbapenemase (KPC)-producing Klebsiella pneumoniae (Kp) are associated with high mortality. The aim of this study is to assess the relationship between time to administration of appropriate antibiotic therapy and the outcome of patients with BSI due to KPC-Kp hospitalized in intensive care unit (ICU).
Methods: An observational study was conducted in the ICUs of two academic centers in Italy. Patients with KPC-Kp bacteremia hospitalized between January 2015 to December 2018 were included. The primary outcome was the relationship between time from blood cultures (BC) collection to appropriate antibiotic therapy and 30-day mortality. The secondary outcome was to evaluate the association of different treatment regimens with 30-day mortality and a composite endpoint (30-day mortality or nephrotoxicity). A Cox regression analysis to identify factors independently associated with 30-day mortality was performed. Hazard ratio (HR) and 95% confidence interval (CI) were calculated.
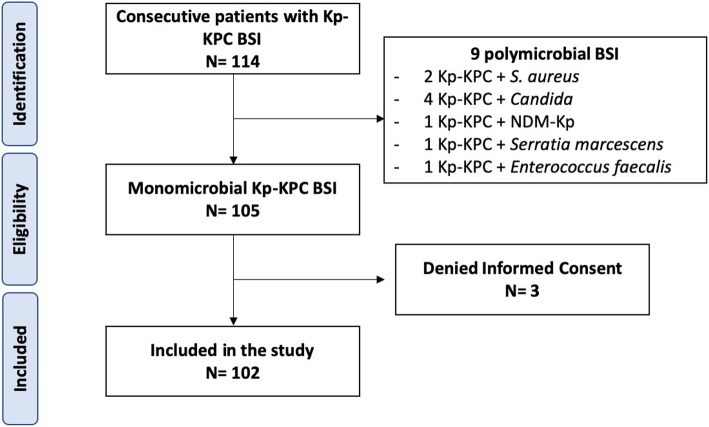
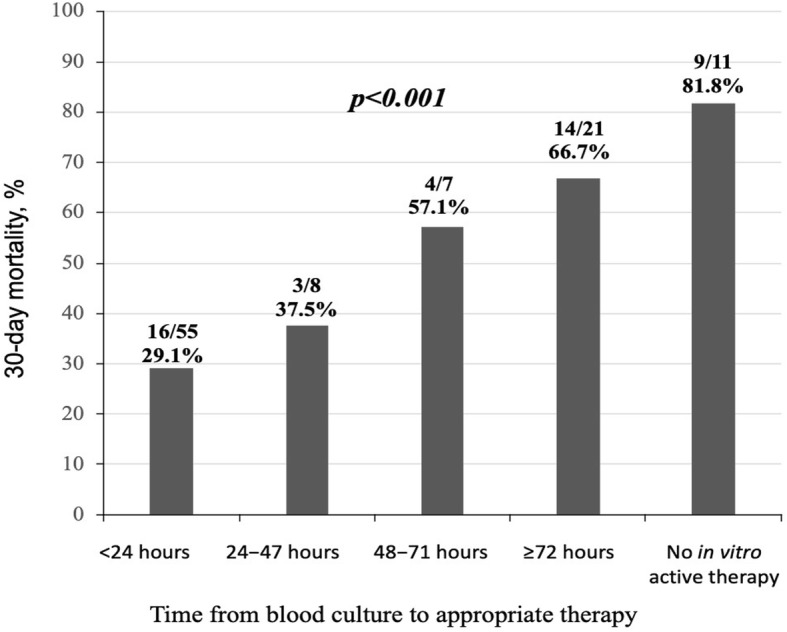
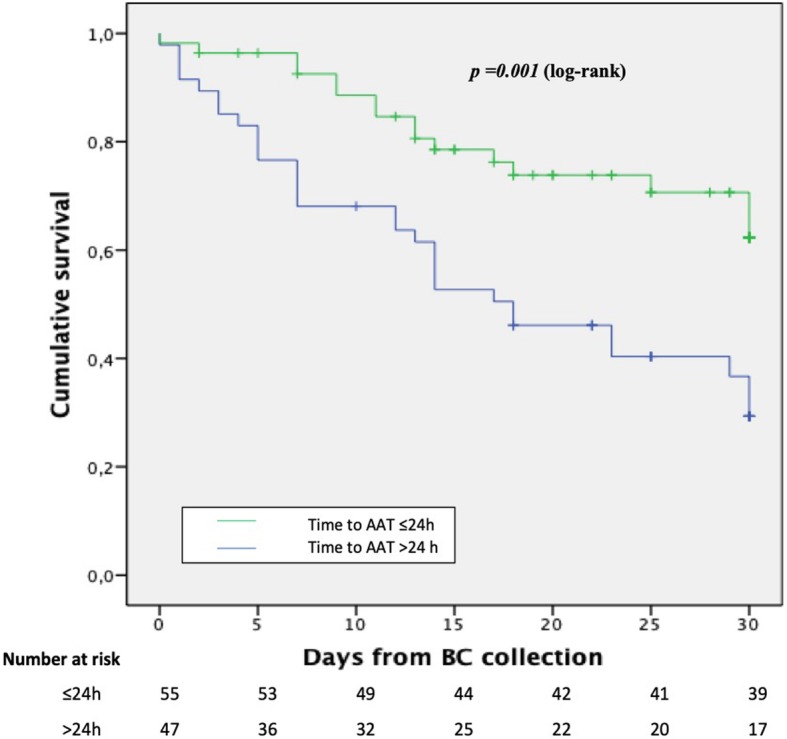
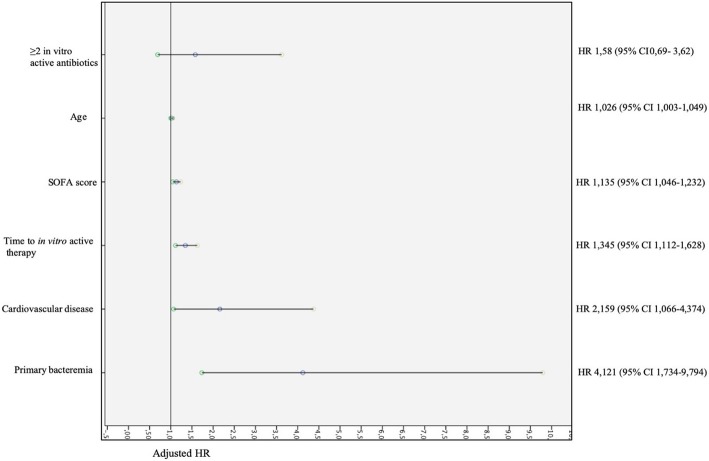
Results: A total of 102 patients with KPC-Kp BSI were included. The most common sources of infection were intra-abdominal (23.5%), urinary tract (20.6%), and skin and skin structure (17.6%). The 30-day mortality was 45%. Median time to appropriate antibiotic therapy was shorter in patients who survived (8.5 h [IQR 1-36]) versus those who died (48 h [IQR 5-108], p = 0.014). A propensity score matching showed that receipt of an in vitro active therapy within 24 h from BC collection was associated with lower 30-day mortality (HR = 0.36, 95% CI: 0.188-0.690, p = 0.0021). At Cox regression analysis, factors associated with 30-day mortality were primary bacteremia (HR 2.662 [95% CI 1.118-6.336], p = 0.027), cardiovascular disease (HR 2.196 [95% CI 1.082-4.457], p = 0.029), time (24-h increments) from BC collection to appropriate therapy (HR 1.382 [95% CI 1.132-1.687], p = 0.001), SOFA score (HR 1.122 [95% CI 1.036-1.216], p = 0.005), and age (HR 1.030 [95% CI 1.006-1.054], p = 0.012). Ceftazidime-avibactam-containing regimens were associated with reduced risk of composite endpoint (30-day mortality OR nephrotoxicity) (HR 0.231 [95% CI 0.071-0.745], p = 0.014) compared to colistin-containing regimens.
Conclusions: Time to appropriate antibiotic therapy is an independent predictor of 30-day mortality in patients with KPC-Kp BSI. Appropriate antibiotic therapy should begin within 24 h from the collection of BC.
Keywords: Antibiotic resistance; Bacteremia; Bloodstream infections; Carbapenem-resistant; Carbapenemases; KPC; Klebsiella pneumoniae; Mortality; Time to appropriate antibiotic therapy.
Conflict of interest statement
MF received grants and was speaker honoraria for MSD, Angelini, Shionogi. FM has participated in advisory boards and/or received speaker honoraria from Angelini, Correvio, MSD, Pfizer, Astellas, Gilead, BMS, Jansenn, ViiV, BioMerieux, Biotest, Becton-Dickinson, Nordic Pharma, Pfizer, Shionogi. MB has participated in advisory boards and/or received speaker honoraria from Achaogen, Angelini, Astellas, AstraZeneca, Bayer, Basilea, Biomerieux, Cepheid, Cidara, Gilead, Menarini, MSD, Paratek, Pfizer, Roche, The Medicine Company, Shionogi, Tetraphase, VenatoRx and Vifor. The remaining authors declare that they have no competing interests.
Figures
References
-
- European Centre for Disease Prevention and Control. Annual report of the European Antimicrobial Resistance Surveillance Network (EARS-Net) (2018). Available from: https://ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-r... Accessed 30 Apr 2019.
-
- European Centre for Disease Prevention and Control. Rapid risk assessment: Carbapenem-resistant Enterobacteriaceae – first update 4 June 2018. Stockholm: ECDC (2018). Available from: https://ecdc.europa.eu/sites/portal/files/documents/RRA-Enterobacteriace.... Accessed 30 Apr 2019.
-
- Cassini A, Högberg LD, Plachouras D, Quattrocchi A, Hoxha A, Simonsen GS, et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European economic area in 2015: a population-level modelling analysis. Lancet Infect Dis. 2019;19:56–66. doi: 10.1016/S1473-3099(18)30605-4. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
