

Role of whole-body MRI for treatment response assessment in multiple myeloma: comparison between clinical response and imaging response
- PMID: 32000858
- PMCID: PMC6993415
- DOI: 10.1186/s40644-020-0293-6
Role of whole-body MRI for treatment response assessment in multiple myeloma: comparison between clinical response and imaging response
Abstract
Background: Whole-body MRI (WB-MRI) including diffusion-weighted image (DWI) have been widely used in patients with multiple myeloma. However, evidence for the value of WB-MRI in the evaluation of treatment response remains sparse. Therefore, we evaluated the role of WB-MRI in the response assessment.
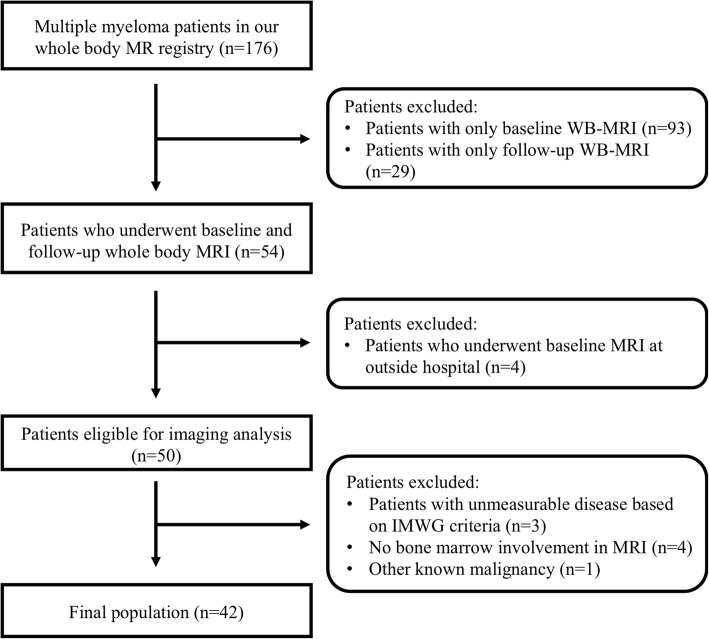
Methods: In our WB-MRI registry, we searched multiple myeloma patients treated with chemotherapy who underwent both baseline and follow-up WB-MRI scans. Clinical responses were categorized as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD), using IMWG criteria. Using RECIST 1.1, MD Anderson (MDA) criteria, and MDA-DWI criteria, imaging responses on WB-MRI were rated as CR, PR, SD, or PD by two radiologists independently. Then, discrepancy cases were resolved by consensus. Weighted Kappa analysis was performed to evaluate agreement between the imaging and clinical responses. The diagnostic accuracy of image responses in the evaluation of clinical CR, objective response (CR and PR), and PD was calculated.
Results: Forty-two eligible patients were included. There was moderate agreement between imaging and clinical responses (κ = 0.54 for RECIST 1.1, κ = 0.58 for MDA criteria, κ = 0.69 for MDA-DWI criteria). WB-MRI showed excellent diagnostic accuracy in assessment of clinical PD (sensitivity 88.9%, specificity 94.7%, positive predictive value [PPV] 84.2%, negative predictive value [NPV] 96.4% in all three imaging criteria). By contrast, WB-MRI showed low accuracy in assessment of clinical CR (sensitivity 4.5%, specificity 98.1%, PPV 50.0%, NPV 71.2% in all three imaging criteria). As to the clinical objective response, the diagnostic accuracy was higher in MDA-DWI criteria than RECIST 1.1 and MDA criteria (sensitivity/specificity/PPV/NPV, 84.2%/94.4%/98.0%/65.4, 54.4%/100%/100%/40.9, and 61.4%/94.4%/97.2%/43.6%, respectively).
Conclusions: In the imaging response assessment of multiple myeloma, WB-MRI showed excellent performance in the evaluation of PD, but not in the assessment of CR or objective response. When adding DWI to imaging response criteria, diagnostic accuracy for objective response was improved and agreement between imaging and clinical responses was increased.
Keywords: Magnetic resonance imaging; Multiple myeloma; Response assessment; Whole-body imaging.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
