

Daratumumab plus lenalidomide and dexamethasone in relapsed/refractory multiple myeloma: extended follow-up of POLLUX, a randomized, open-label, phase 3 study
- PMID: 32001798
- PMCID: PMC7326710
- DOI: 10.1038/s41375-020-0711-6
Daratumumab plus lenalidomide and dexamethasone in relapsed/refractory multiple myeloma: extended follow-up of POLLUX, a randomized, open-label, phase 3 study
Abstract
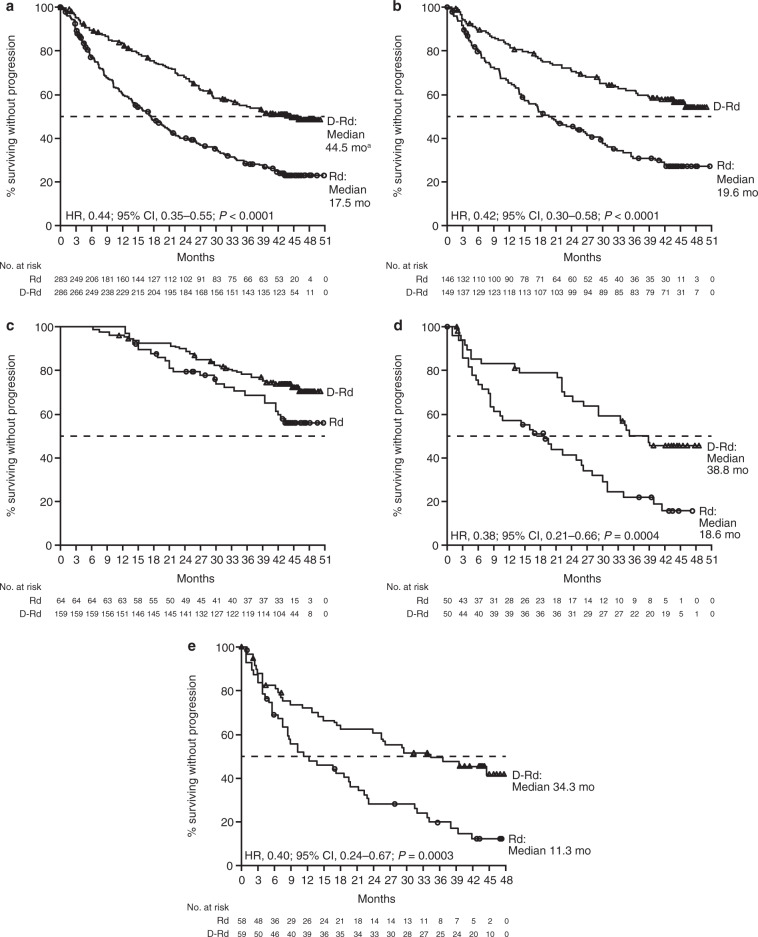
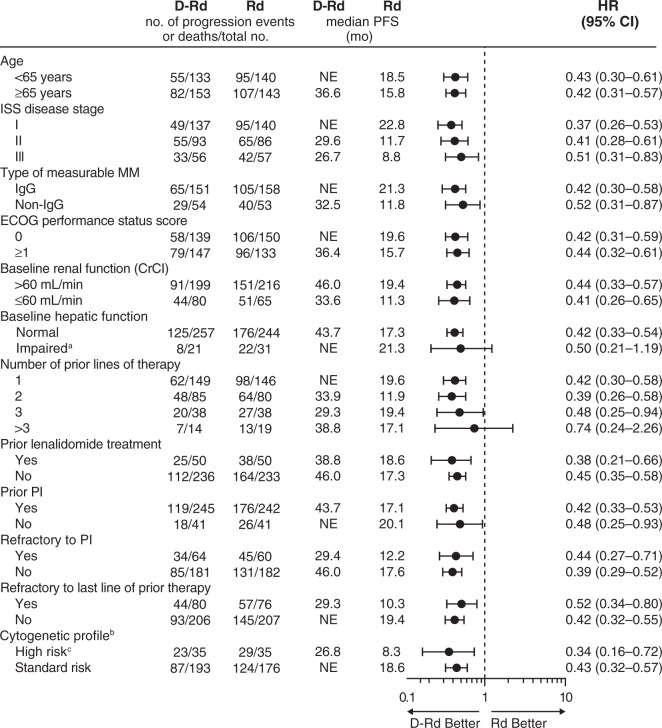
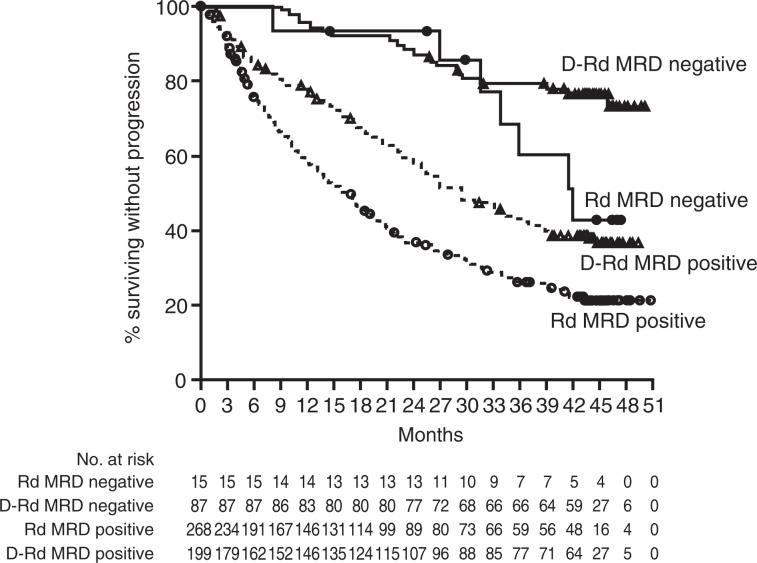
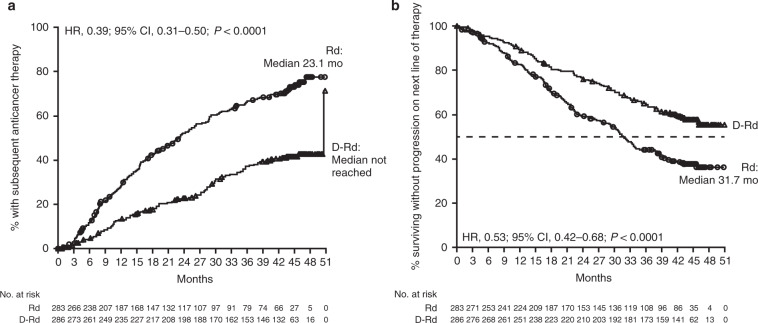
In POLLUX, daratumumab (D) plus lenalidomide/dexamethasone (Rd) reduced the risk of disease progression or death by 63% and increased the overall response rate (ORR) versus Rd in relapsed/refractory multiple myeloma (RRMM). Updated efficacy and safety after >3 years of follow-up are presented. Patients (N = 569) with ≥1 prior line received Rd (lenalidomide, 25 mg, on Days 1-21 of each 28-day cycle; dexamethasone, 40 mg, weekly) ± daratumumab at the approved dosing schedule. Minimal residual disease (MRD) was assessed by next-generation sequencing. After 44.3 months median follow-up, D-Rd prolonged progression-free survival (PFS) in the intent-to-treat population (median 44.5 vs 17.5 months; HR, 0.44; 95% CI, 0.35-0.55; P < 0.0001) and in patient subgroups. D-Rd demonstrated higher ORR (92.9 vs 76.4%; P < 0.0001) and deeper responses, including complete response or better (56.6 vs 23.2%; P < 0.0001) and MRD negativity (10-5; 30.4 vs 5.3%; P < 0.0001). Median time to next therapy was prolonged with D-Rd (50.6 vs 23.1 months; HR, 0.39; 95% CI, 0.31-0.50; P < 0.0001). Median PFS on subsequent line of therapy (PFS2) was not reached with D-Rd versus 31.7 months with Rd (HR, 0.53; 95% CI, 0.42-0.68; P < 0.0001). No new safety concerns were reported. These data support using D-Rd in patients with RRMM after first relapse.
Conflict of interest statement
NJB consulted for and received honoraria and research funding from Janssen, Celgene, and Amgen. MAD consulted for and received honoraria from Janssen, Celgene, Takeda, Amgen, and Bristol-Myers Squibb. DJW received honoraria from and served on advisory committees for Amgen, Celgene, Janssen, and Takeda. GC received honoraria from Amgen, Bristol-Myers Squibb, GlycoMimetics, Celgene, Janssen, Takeda, and Sanofi; and received research funding from Celgene, Janssen, and Takeda. PJH received honoraria from Janssen, Amgen, Novartis, and Takeda; and received travel support from Takeda and Celgene. PM received honoraria from and served on advisory committees for Amgen, Celgene, Janssen, Takeda, and AbbVie. JLK served in a consulting or advisory role for Janssen, Celgene, Takeda, Amgen, and Sanofi Genzyme; and received research funding from Janssen, Bluebird, Bristol-Myers Squibb, Celgene, and Sutro Biopharma. MK, CC, XQ, LO, ST, JU, and MQ are employees of Janssen. JS-M received honoraria from Janssen, Celgene, Amgen, Bristol-Myers Squibb, Novartis, Sanofi, and Roche. LB, ML, KK, and NT have no conflicts of interest to disclose.
Figures
References
-
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology™. Multiple Myeloma. Version 1.2019. 2018. https://www.nccn.org/professionals/physician_gls/pdf/myeloma.pdf. Accessed 19 Oct 2018.
-
- Lammerts van Bueren J, Jakobs D, Kaldenhoven N, Roza M, Hiddingh S, Meesters J, et al. Direct in vitro comparison of daratumumab with surrogate analogs of CD38 antibodies MOR03087, SAR650984 and Ab79. Blood. 2014;124:3474. doi: 10.1182/blood.V124.21.3474.3474. - DOI
-
- Overdijk MB, Verploegen S, Bogels M, van Egmond M, Lammerts van Bueren JJ, Mutis T, et al. Antibody-mediated phagocytosis contributes to the anti-tumor activity of the therapeutic antibody daratumumab in lymphoma and multiple myeloma. MAbs. 2015;7:311–21. doi: 10.1080/19420862.2015.1007813. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
