

Tracking the evolution of circulating exosomal-PD-L1 to monitor melanoma patients
- PMID: 32002173
- PMCID: PMC6968537
- DOI: 10.1080/20013078.2019.1710899
Tracking the evolution of circulating exosomal-PD-L1 to monitor melanoma patients
Abstract
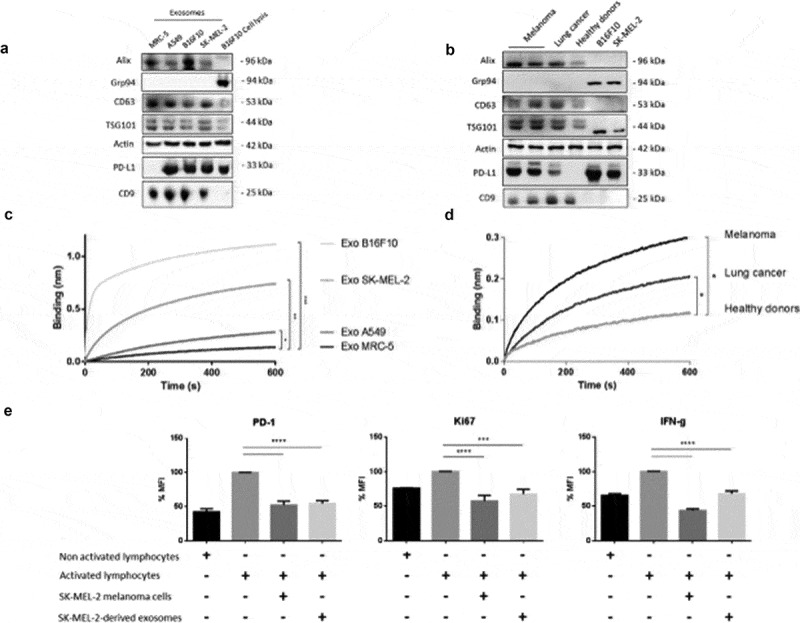
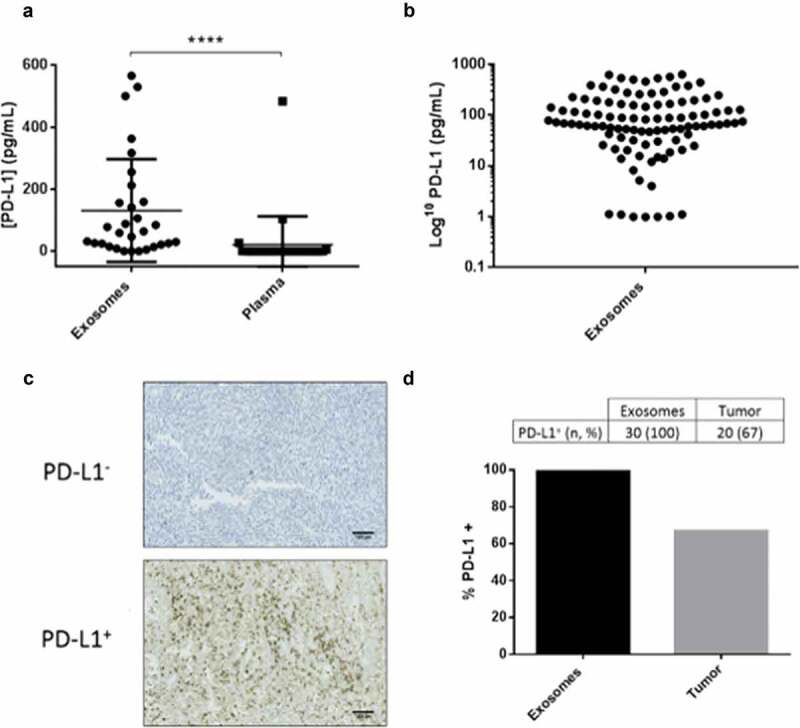
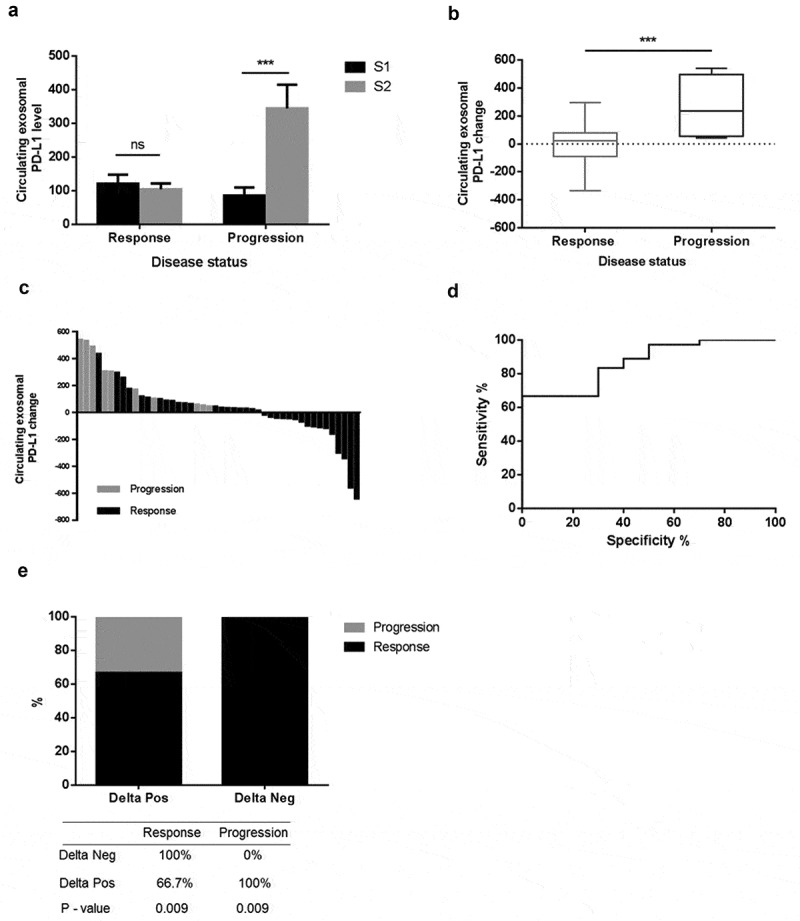
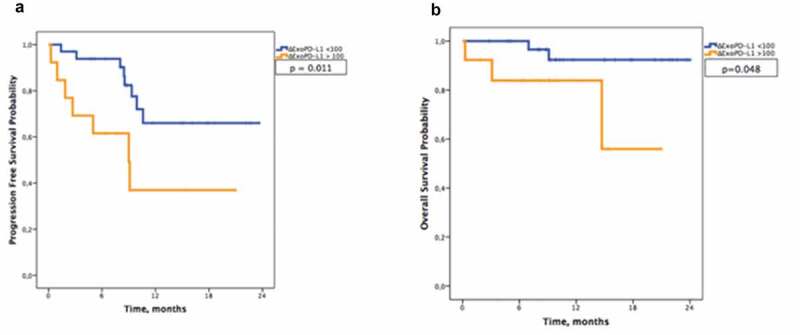
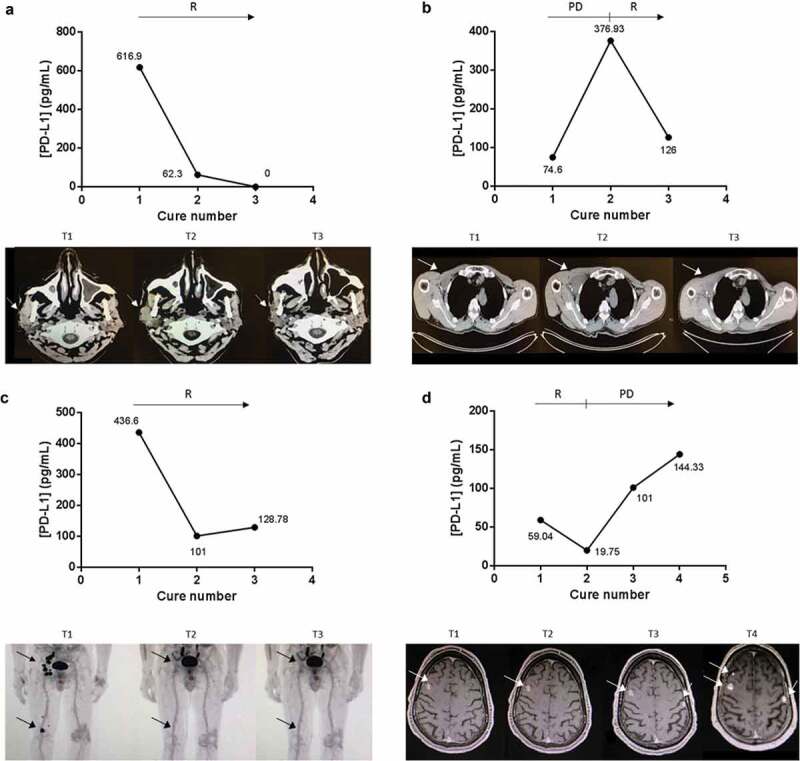
In the era of immunotherapies there is an urgent need to implement the use of circulating biomarkers in clinical practice to facilitate personalized therapy and to predict treatment response. We conducted a prospective study to evaluate the usefulness of circulating exosomal-PD-L1 in melanoma patients' follow-up. We studied the dynamics of exosomal-PD-L1 from 100 melanoma patients by using an enzyme-linked immunosorbent assay. We found that PD-L1 was secreted through exosomes by melanoma cells. Exosomes carrying PD-L1 had immunosuppressive properties since they were as efficient as the cancer cell from which they derive at inhibiting T-cell activation. In plasma from melanoma patients, the level of PD-L1 (n= 30, median 64.26 pg/mL) was significantly higher in exosomes compared to soluble PD-L1 (n= 30, 0.1 pg/mL). Furthermore, exosomal-PD-L1 was detected in all patients whereas only 67% of tumour biopsies were PD-L1 positive. Although baseline exosomal-PD-L1 levels were not associated with clinic-pathologic characteristics, their variations after the cures (ΔExoPD-L1) correlated with the tumour response to treatment. A ΔExoPD-L1 cut-off of> 100 was defined, yielding an 83% sensitivity, a 70% specificity, a 91% positive predictive value and 54% negative predictive values for disease progression. The use of the cut-off allowed stratification in two groups of patients statistically different concerning overall survival and progression-free survival. PD-L1 levels in circulating exosomes seem to be a more reliable marker than PD-L1 expression in tumour biopsies. Monitoring of circulating exosomal-PD-L1 may be useful to predict the tumour response to treatment and clinical outcome.
Keywords: Melanoma; PD-L1/PD-1; exosome; follow-up; immune checkpoint.
© 2020 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group.
Conflict of interest statement
No potential conflict of interest was reported by the authors.
Figures
References
-
- Ribas A, Hamid O, Daud A, et al. Association of pembrolizumab with tumor response and survival among patients with advanced melanoma. JAMA. 2016. April 19;315(15):1600–1609. - PubMed
-
- Robert C, Long GV, Brady B, et al. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med. 2015. January 22;372(4):320–330. - PubMed
-
- Madore J, Vilain RE, Menzies AM, et al. PD-L1 expression in melanoma shows marked heterogeneity within and between patients: implications for anti-PD-1/PD-L1 clinical trials. Pigment Cell Melanoma Res. 2015. May;28(3):245–253. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials
