

Evaluating the role of FAMIly history of cancer and diagnosis of multiple neoplasms in cancer patients receiving PD-1/PD-L1 checkpoint inhibitors: the multicenter FAMI-L1 study
- PMID: 32002308
- PMCID: PMC6959456
- DOI: 10.1080/2162402X.2019.1710389
Evaluating the role of FAMIly history of cancer and diagnosis of multiple neoplasms in cancer patients receiving PD-1/PD-L1 checkpoint inhibitors: the multicenter FAMI-L1 study
Abstract
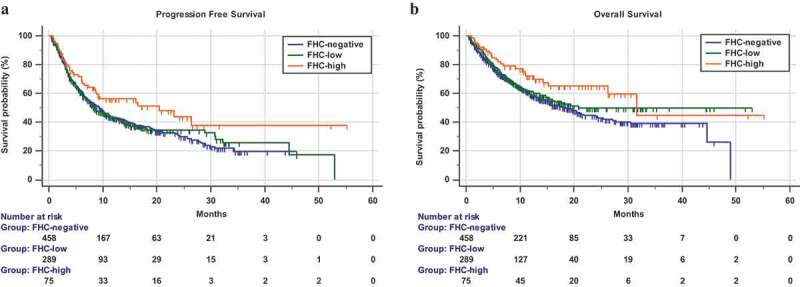
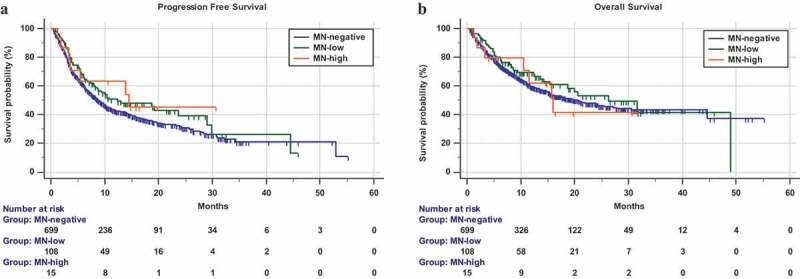
Background: We investigate the role of family history of cancer (FHC) and diagnosis of metachronous and/or synchronous multiple neoplasms (MN), during anti-PD-1/PD-L1 immunotherapy. Design: This was a multicenter retrospective study of advanced cancer patients treated with anti-PD-1/PD-L1 immunotherapy. FHC was collected in lineal and collateral lines, and patients were categorized as follows: FHC-high (in case of cancer diagnoses in both the lineal and collateral family lines), FHC-low (in case of cancer diagnoses in only one family line), and FHC-negative. Patients were also categorized according to the diagnosis of MN as follows: MN-high (>2 malignancies), MN-low (two malignancies), and MN-negative. Objective response rate (ORR), progression-free survival (PFS), overall survival (OS), and incidence of immune-related adverse events (irAEs) of any grade were evaluated. Results: 822 consecutive patients were evaluated. 458 patients (55.7%) were FHC-negative, 289 (35.2%) were FHC-low, and 75 (9.1%) FHC-high, respectively. 29 (3.5%) had a diagnosis of synchronous MN and 94 (11.4%) of metachronous MN. 108 (13.2%) and 15 (1.8%) patients were MN-low and MN-high, respectively. The median follow-up was 15.6 months. No significant differences were found regarding ORR among subgroups. FHC-high patients had a significantly longer PFS (hazard ratio [HR] = 0.69 [95% CI: 0.48-0.97], p = .0379) and OS (HR = 0.61 [95% CI: 0.39-0.93], p = .0210), when compared to FHC-negative patients. FHC-high was confirmed as an independent predictor for PFS and OS at multivariate analysis. No significant differences were found according to MN categories. FHC-high patients had a significantly higher incidence of irAEs of any grade, compared to FHC-negative patients (p = .0012). Conclusions: FHC-high patients seem to benefit more than FHC-negative patients from anti-PD-1/PD-L1 checkpoint inhibitors.
Keywords: DDR genes; Family history of cancer; PD-1; immune checkpoint inhibitors; immunotherapy; multiple neoplasms.
© 2020 The Author(s). Published with license by Taylor & Francis Group, LLC.
Figures
References
-
- Taube JM, Klein A, Brahmer JR, Xu H, Pan X, Kim JH, Chen L, Pardoll DM, Topalian SL, Anders RA, et al. Association of PD-1, PD-1 ligands, and other features of the tumor immune microenvironment with response to anti-PD-1 therapy. Clin Cancer Res. 2014;20(19):5064–10. doi: 10.1158/1078-0432.CCR-13-3271. - DOI - PMC - PubMed
-
- Hellmann MD, Ciuleanu T-E, Pluzanski A, Lee JS, Otterson GA, Audigier-Valette C, Minenza E, Linardou H, Burgers S, Salman P, et al. Nivolumab plus ipilimumab in lung cancer with a high tumor mutational burden. N Engl J Med. 2018. May 31;378(22):2093–2104. doi: 10.1056/NEJMoa1801946. Epub 2018 Apr 16. - DOI - PMC - PubMed
-
- Cortellini A, Bersanelli M, Buti S, Cannita K, Santini D, Perrone F, Giusti R, Tiseo M, Michiara M, Di Marino P, et al. A multicenter study of body mass index in cancer patients treated with anti-PD-1/PD-L1 immune checkpoint inhibitors: when overweight becomes favorable. J Immuno Ther Cancer. 2019. February 27;7(1):57. doi: 10.1186/s40425-019-0527-y. - DOI - PMC - PubMed
-
- Routy B, Le Chatelier E, Derosa L, Duong CPM, Alou MT, Daillère R, Fluckiger A, Messaoudene M, Rauber C, Roberti MP, et al. Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science. 2018. January 5;359(6371):91–97. doi: 10.1126/science.aan3706. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials