

Cost Analysis of Single-Level Lumbar Fusions
- PMID: 32002348
- PMCID: PMC6963351
- DOI: 10.1177/2192568219853251
Cost Analysis of Single-Level Lumbar Fusions
Abstract
Study design: Cost analysis of a retrospectively identified cohort of patients who had undergone primary single-level lumbar fusion at a single institution's orthopedic or neurosurgery department.
Objective: The purpose of this article is to analyze the determinants of direct costs for single-level lumbar fusions and identify potential areas for cost reduction.
Methods: Adult patients who underwent primary single-level lumbar fusion from fiscal years 2008 to 2012 were identified via administrative and departmental databases and were eligible for inclusion. Patients were excluded if they underwent multiple surgeries, had previous surgery at the same anatomic region, underwent corpectomy, kyphectomy, disc replacement, surgery for tumor or infection, or had incomplete cost data. Demographic data, surgical data, and direct cost data in the categories of supplies, services, room and care, and pharmacy, was collected for each patient.
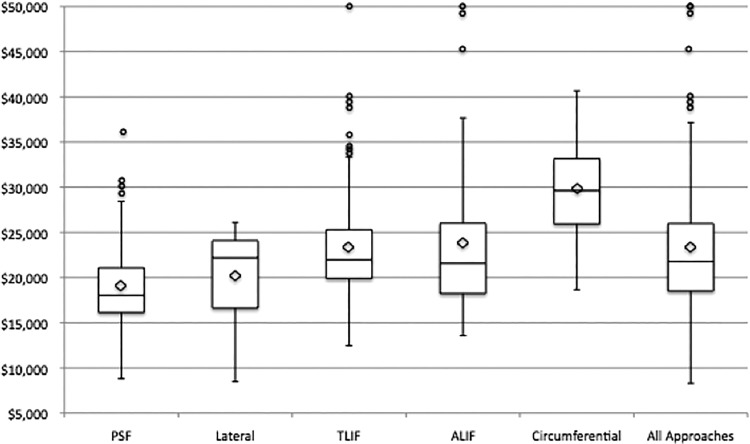
Results: The cohort included 532 patients. Direct costs ranged from $8286 to $73 727 (median = $21 781; mean = $22 890 ± $6323). Surgical approach was an important determinant of cost. The mean direct cost was highest for the circumferential approach and lowest for posterior instrumented spinal fusions without an interbody cage. The difference in mean direct cost between transforaminal lumbar interbody fusions, anterior lumbar interbody fusions, and lateral transpsoas fusions was not statistically significant. Surgical supplies accounted for 44% of direct costs. Spinal implants were the primary component of supply costs (84.9%). Services accounted for 38% of direct costs and were highly dependent on operative time. Comorbidities were an important contributor to variance in the cost of care as evidenced by high variance in pharmacy costs and length of stay related to their management.
Conclusion: The costs of spinal surgeries are highly variable. Important cost drivers in our analysis included surgical approach, implants, operating room time, and length of hospital stay. Areas of high cost and high variance offer potential targets for cost savings and quality improvements.
Keywords: economic evaluation; health care spending; lumbar; single-level; spinal fusion; spine surgery.
© The Author(s) 2019.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Martin BI, Deyo RA, Mirza SK, et al. Expenditures and health status among adults with back and neck problems. JAMA. 2008;299:656–664. - PubMed
-
- Katz JN. Lumbar spinal fusion. Surgical rates, costs, and complications. Spine (Phila Pa 1976). 1995;20(24 suppl):78S–83S. - PubMed
-
- Deyo RA, Gray DT, Kreuter W, Mirza S, Martin BI. United States trends in lumbar fusion surgery for degenerative conditions. Spine (Phila Pa 1976). 2005;30:1441–1445. - PubMed
-
- United States Bone and Joint Initiative. The Burden of Musculoskeletal Diseases in the United States. 2nd ed Rosemont, IL: American Academy of Orthopaedic Surgeons; 2011.
-
- Abraham DJ, Herkowitz HN, Katz JN. Indications for thoracic and lumbar spine fusion and trends in use. Orthop Clin North Am. 1998;29:803. - PubMed
