

Minimal ablative margin (MAM) assessment with image fusion: an independent predictor for local tumor progression in hepatocellular carcinoma after stereotactic radiofrequency ablation
- PMID: 32002642
- PMCID: PMC7160081
- DOI: 10.1007/s00330-019-06609-7
Minimal ablative margin (MAM) assessment with image fusion: an independent predictor for local tumor progression in hepatocellular carcinoma after stereotactic radiofrequency ablation
Abstract
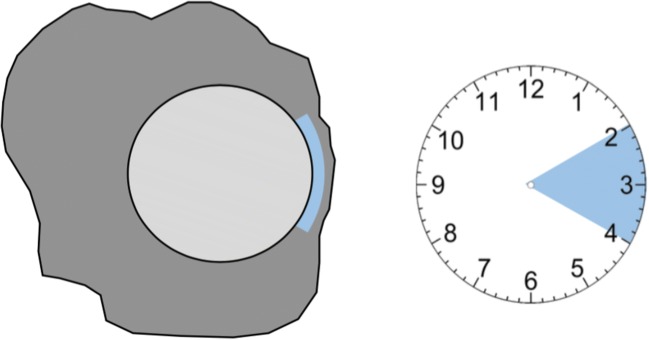
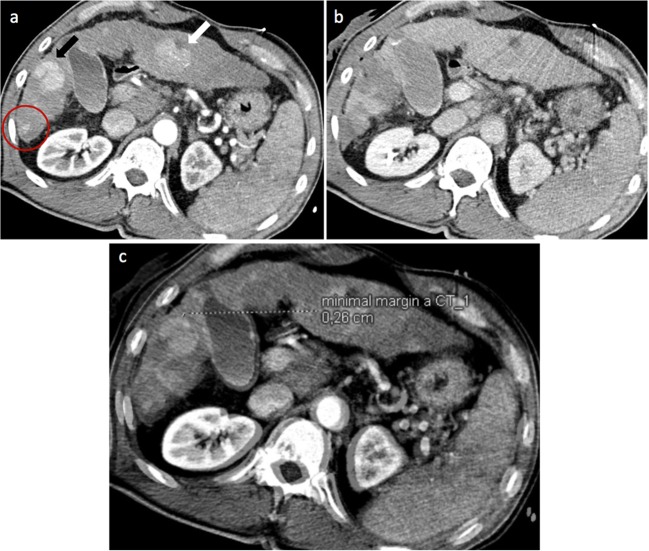
Objectives: To assess the minimal ablative margin (MAM) by image fusion of intraprocedural pre- and post-ablation contrast-enhanced CT images and to evaluate if it can predict local tumor progression (LTP) independently. Furthermore, to determine a MAM with which a stereotactic radiofrequency ablation (SRFA) can be determined successful and therefore used as an intraprocedural tool to evaluate treatment success.
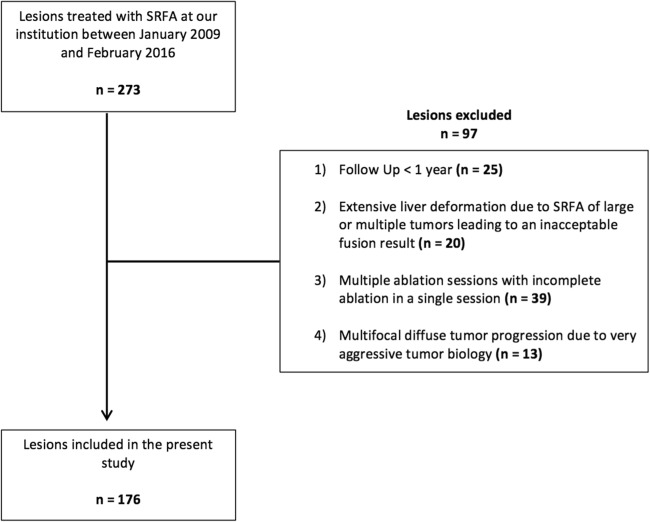
Methods: A total of 110 patients (20 women, 90 men; mean age 63.7 ± 10.2) with 176 hepatocellular carcinomas were assessed by retrospective analysis of prospectively collected data. The MAM was determined through image fusion of intraprocedural pre- and post-ablation images using commercially available rigid imaging registration software. LTP was assessed in contrast-enhanced CTs or MR scans at 3-6-month intervals.
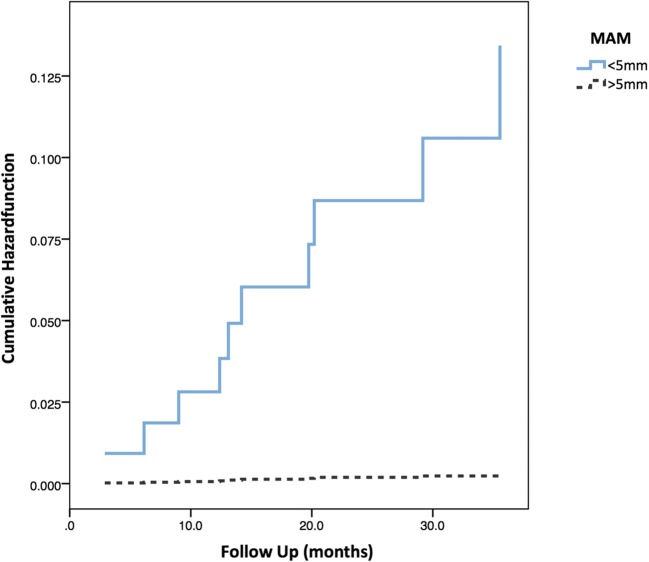
Results: The MAM was the only significant independent predictor of LTP (p = 0.036). For each millimeter increase of the MAM, a 30% reduction of the relative risk for LTP was found (OR = 0.7, 95% CI 0.5-0.98, p = 0.036). No LTP was detected in lesions with a MAM > 5 mm. The overall LTP rate was 9 of 110 (8.2%) on a patient level and 10 of 173 (5.7%) on a lesion level. The median MAM was 3.4 (1.7-6.9) mm. The mean overall follow-up period was 26.0 ± 10.3 months.
Conclusions: An immediate assessment of the minimal ablative margin (MAM) can be used as an intraprocedural tool to evaluate the treatment success in patients treated with stereotactic RFA. A MAM > 5 mm has to be achieved to consider an ablation as successful.
Key points: • An intraoperatively measured minimal ablative margin (MAM) > 5 mm correlates with complete remission. • MAM is the only significant independent predictor of LTP (OR = 0.7, 95% CI 0.5-0.98, p = 0.036) after stereotactic RFA of hepatocellular carcinoma. • Image fusion using commercially available rigid imaging registration software is possible, even though considerably complex. Therefore, improved (semi-)automatic fusion software is highly desirable.
Keywords: Ablation techniques; Carcinoma, hepatocellular; Radiofrequency ablation; Tomography, X-ray computed; Treatment outcome.
Conflict of interest statement
Reto Bale is a consultant of CASCINATION. Amilcar Alzaga is an employee of Siemens Healthineers.
The other authors do not have any conflicts of interest to disclose.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
