

Facility Variability in Examination Indication Among Women With Prior Breast Cancer: Implications and the Need for Standardization
- PMID: 32004483
- PMCID: PMC7275918
- DOI: 10.1016/j.jacr.2019.12.020
Facility Variability in Examination Indication Among Women With Prior Breast Cancer: Implications and the Need for Standardization
Abstract
Objective: We sought to identify and characterize examinations in women with a personal history of breast cancer likely performed for asymptomatic surveillance.
Methods: We included surveillance mammograms (1997-2017) in asymptomatic women with a personal history of breast cancer diagnosed at age ≥18 years (1996-2016) from 103 Breast Cancer Surveillance Consortium facilities. We examined facility-level variability in examination indication. We modeled the relative risk (RR) and 95% confidence intervals (CIs) at the examination level of a (1) nonscreening indication and (2) surveillance interval ≤9 months using Poisson regression with fixed effects for facility, stage, diagnosis age, surgery, examination year, and time since diagnosis.
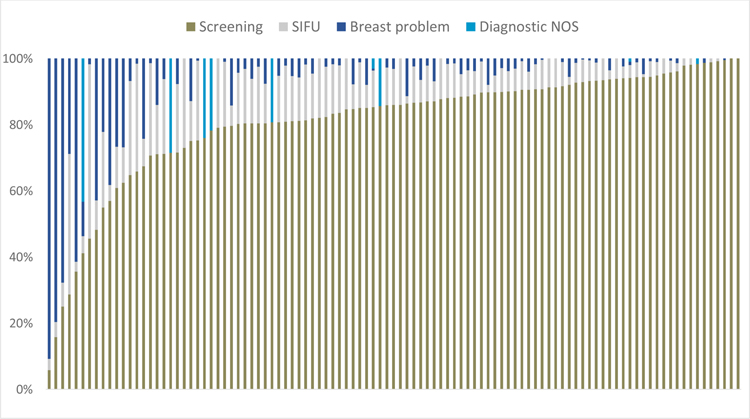
Results: Among 244,855 surveillance mammograms, 69.5% were coded with a screening indication, 12.7% short-interval follow-up, and 15.3% as evaluation of a breast problem. Within a facility, the proportion of examinations with a screening indication ranged from 6% to 100% (median 86%, interquartile range 79%-92%). Facilities varied the most for examinations in the first 5 years after diagnosis, with 39.4% of surveillance mammograms having a nonscreening indication. Within a facility, breast conserving surgery compared with mastectomy (RR = 1.64; 95% CI = 1.60-1.68) and less time since diagnosis (1 year versus 5 years; RR = 1.69; 95% CI = 1.66-1.72; 3 years versus 5 years = 1.20; 95% CI = 1.18-1.23) were strongly associated with a nonscreening indication with similar results for ≤9-month surveillance interval. Screening indication and >9-month surveillance intervals were more common in more recent years.
Conclusion: Variability in surveillance indications across facilities in the United States supports including indications beyond screening in studies evaluating surveillance mammography effectiveness and demonstrates the need for standardization.
Keywords: Breast Cancer Surveillance Consortium; Breast cancer screening; breast cancer surveillance; breast carcinoma; mammography indication.
Copyright © 2020. Published by Elsevier Inc.
Figures



References
-
- American Cancer Society. Breast Cancer Detailed Guide - What are the Key Statistics About Breast Cancer? 2016. [updated May 4, 2016. Available from: http://www.cancer.org/cancer/breastcancer/detailedguide/breast-cancer-ke....
-
- Runowicz CD, Leach CR, Henry NL, Henry KS, Mackey HT, Cowens-Alvarado RL, et al. American Cancer Society/American Society of Clinical Oncology Breast Cancer Survivorship Care Guideline. J Clin Oncol. 2016;34(6):611–35. - PubMed
-
- Moy L, Newell MS, Mahoney MC, Bailey L, Barke LD, Carkaci S, et al. ACR Appropriateness Criteria stage I breast cancer: initial workup and surveillance for local recurrence and distant metastases in asymptomatic women. J Am Coll Radiol. 2014;11(12 Pt A):1160–8. - PubMed
-
- Khatcheressian JL, Hurley P, Bantug E, Esserman LJ, Grunfeld E, Halberg F, et al. Breast cancer follow-up and management after primary treatment: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2013;31(7):961–5. - PubMed
-
- National Comprehensive Cancer Network (NCCN). Clinical Practice Guidelines in Oncology - Breast Cancer Fort Washington, PA: National Comprehensive Cancer Network (NCCN); 2016. [Clinical Practice Guidelines in Oncology - Breast Cancer, Version 1.2016. :[Available from: http://nccn.org. - PubMed
